Department of Infectious Diseases and Hepatology, Pomeranian Medical University, Szczecin, Poland.
PLoS One. 2011;6(7):e22215. doi: 10.1371/journal.pone.0022215. Epub 2011 Jul 18.
Investigation of the interplay between the CCR5 Δ32/wt genotype and demographic, epidemiological, clinical and immunological factors associated with mortality in the cART era.
Longitudinal data from 507 HIV-infected patients following the Δ32 allele detection were analyzed.
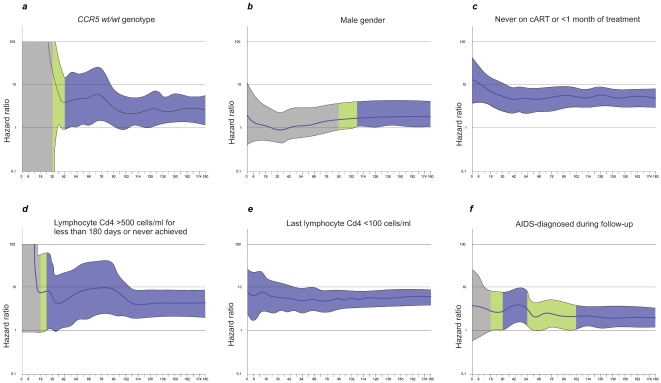
Cumulative 15 years mortality was calculated using Kaplan-Meyer methodology. Hazard ratios were estimated using univariate Cox models. Basing on Akakie information criteria and statistical significance multivariate Cox model was constructed and effect plots presenting adjusted hazard ratio time-dependency were drawn. Analysis of the association of all-cause mortality and CCR5 Δ32/wt genotype prior to the antiretroviral treatment (cART) initiation (n = 507) and on the therapy (n = 422) was also performed.
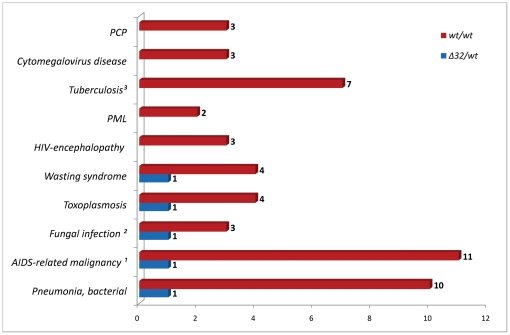
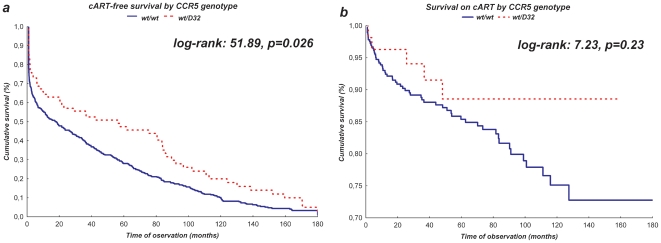
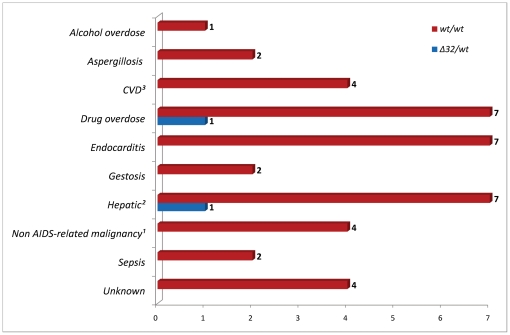
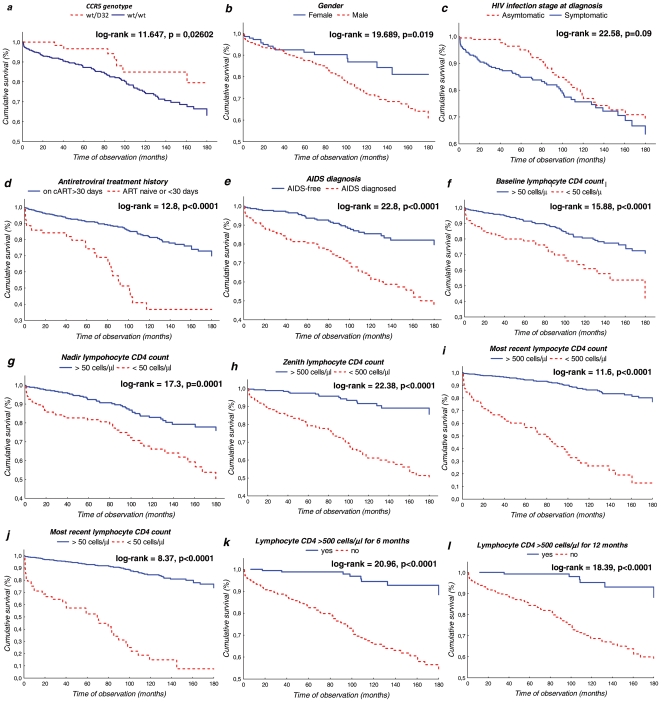
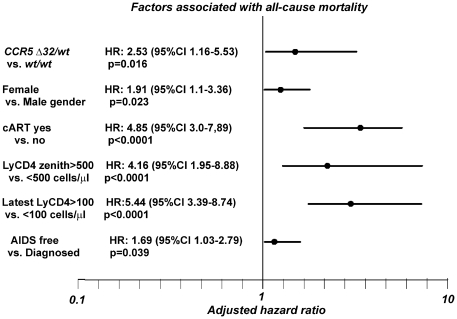
A mortality rate of 2.66 (CI 2.57-3.19) per 100 person-years was observed. Univariate analysis factors modifying the risk of death included the CCR5 genotype, gender, history of cART, AIDS diagnosis and also CD4 lymphocyte nadir, zenith, the latest CD4 count and stable levels >500 cells/µl. For multivariate analysis the following predictors were selected: CCR5 genotype (HR for wt/wt 2.53, CI 1.16-5.53, p = 0.02), gender (HR for males 1.91, 95%CI 1.1-3.36, p = 0.023), introduction of combined antiretroviral treatment (HR 4.85, CI 3.0-7.89, if untreated or treated <1 month, p<0.0001) CD4 count of 500 cells/µl for six months or more (HR 4.16, CI 1.95-8.88 if not achieved, p = 0.028), the latest CD4 count (HR 5.44, CI 3.39-8.74 for <100 cells/µl, p<0.0001) and history of AIDS (HR 1.69, CI 1.03-2.79, p = 0.039). Among untreated individuals the Δ32/wt genotype was associated with notably better survival (p = 0.026), while among cART treated individuals the Δ32 mutation did not correlate significantly with higher survival rates (p = 0.23).
The Δ32 CCR5 allele is associated with a reduction of the risk of all-cause mortality in HIV (+) patients alongside clinical and immunologic predictors such as AIDS, history of cART, lymphocyte CD4 cell count and gender.
探讨 CCR5Δ32/wt 基因型与 cART 时代与死亡率相关的人口统计学、流行病学、临床和免疫学因素之间的相互作用。
对 507 例检测到Δ32 等位基因的 HIV 感染患者的纵向数据进行了分析。
使用 Kaplan-Meier 方法计算了 15 年的累计死亡率。使用单变量 Cox 模型估计风险比。基于赤池信息量准则和统计学意义,构建了多变量 Cox 模型,并绘制了呈现调整后风险比时间依赖性的效应图。还分析了在开始抗逆转录病毒治疗 (cART) 之前(n = 507)和治疗期间(n = 422)所有原因死亡率与 CCR5Δ32/wt 基因型的相关性。
观察到每 100 人年 2.66(CI 2.57-3.19)的死亡率。单变量分析中,改变死亡风险的因素包括 CCR5 基因型、性别、cART 史、艾滋病诊断以及 CD4 淋巴细胞最低点、最高点和最新 CD4 计数以及稳定水平>500 个细胞/µl。多变量分析中选择了以下预测因子:CCR5 基因型(wt/wt 为 2.53,CI 1.16-5.53,p = 0.02)、性别(男性为 1.91,95%CI 1.1-3.36,p = 0.023)、联合抗逆转录病毒治疗的引入(未治疗或治疗<1 个月时为 4.85,CI 3.0-7.89,p<0.0001)、CD4 计数 500 个细胞/µl 持续 6 个月或更长时间(未达到时为 4.16,CI 1.95-8.88,p = 0.028)、最新 CD4 计数(<100 个细胞/µl 时为 5.44,CI 3.39-8.74,p<0.0001)和艾滋病史(HR 1.69,CI 1.03-2.79,p = 0.039)。在未治疗的个体中,Δ32/wt 基因型与显著更好的生存相关(p = 0.026),而在接受 cART 治疗的个体中,Δ32 突变与更高的生存率无显著相关性(p = 0.23)。
在 HIV(+)患者中,Δ32 CCR5 等位基因与 AIDS、cART 史、淋巴细胞 CD4 细胞计数和性别等临床和免疫预测因子一起,与全因死亡率降低相关。