Division of Hepatobiliary, Pancreatic, and Gastrointestinal Surgery, Department of Surgery, Washington University School of Medicine, St. Louis, MO 63110, USA.
Surgery. 2011 Aug;150(2):169-76. doi: 10.1016/j.surg.2011.05.012.
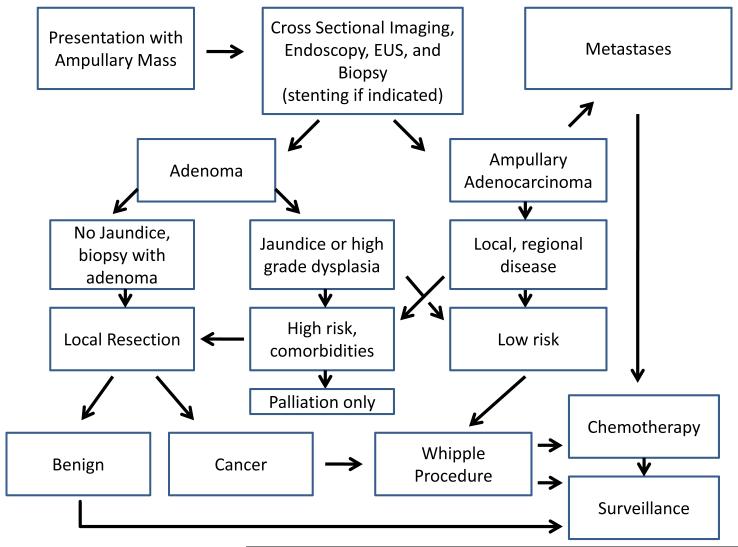
Although benign ampullary tumors are removed endoscopically, due to their potential to progress to malignant disease, the favored treatment for adenocarcinoma is pancreaticoduodenectomy. We reviewed our institution's experience in order to identify which patients were at highest risk of disease progression following surgical resection, as well as evaluate whether localized T1 tumors are best treated by pancreaticoduodenectomy.
We retrospectively reviewed 157 patients who presented with an ampullary mass, from 2001 to 2010, and identified 51 with benign adenoma and 106 with adenocarcinoma.
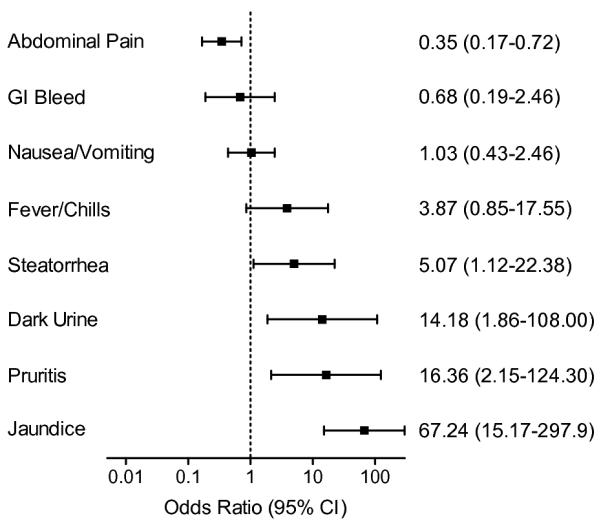
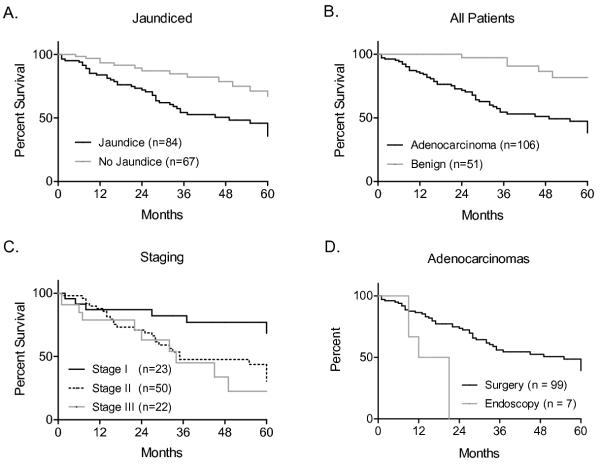
Patients with malignant tumors most often presented with larger tumors and jaundice, which alone was predictive of survival (OR = 67). Forty-five percent of patients with pathologically confirmed T1 tumors had positive lymph nodes and median survival was modest at 60 months. Lymph node involvement was predictive of recurrence and decreased survival.
Patients with malignant tumors often present with jaundice and larger tumors. These findings should warrant suspicion for cancer and expedited preoperative workup. Based on our finding that nearly half the patients with T1 tumors had positive lymph nodes, we recommend pancreaticoduodenectomy for any patient with biopsy proven adenocarcinoma who is a suitable candidate for surgery.
虽然良性壶腹肿瘤可以通过内镜切除,但由于其有进展为恶性疾病的潜在风险,腺癌的首选治疗方法是胰十二指肠切除术。我们回顾了我们机构的经验,以确定哪些患者在手术后疾病进展的风险最高,并评估局部 T1 肿瘤是否最好通过胰十二指肠切除术治疗。
我们回顾性分析了 2001 年至 2010 年间就诊的 157 例壶腹肿块患者,其中 51 例为良性腺瘤,106 例为腺癌。
恶性肿瘤患者常表现为更大的肿瘤和黄疸,而这两项单独就可预测生存(OR = 67)。45%的病理证实为 T1 肿瘤的患者有阳性淋巴结,中位生存期仅为 60 个月。淋巴结受累可预测复发和降低生存率。
恶性肿瘤患者常伴有黄疸和较大的肿瘤。这些发现应引起对癌症的怀疑,并加快术前检查。根据我们发现近一半 T1 肿瘤患者有阳性淋巴结的结果,我们建议对任何有活检证实的腺癌且适合手术的患者进行胰十二指肠切除术。