Dusick Joshua R, Evans Brandon C, Laiwalla Azim, Krahl Scott, Gonzalez Nestor R
Department of Neurosurgery, UCLA David Geffen School of Medicine, Los Angeles, CA, USA.
Surg Neurol Int. 2011;2:99. doi: 10.4103/2152-7806.83023. Epub 2011 Jul 18.
Double-injection models of subarachnoid hemorrhage (SAH) in rats are the most effective in producing vasospasm, delayed neurological deficits and infarctions. However, they require two large surgeries to expose the femoral artery and the atlanto-occipital membrane. We have developed a minimally-invasive modification that prevents confounding effects of surgical procedures, leakage of blood from the subarachnoid space and minimizes risk of infection.
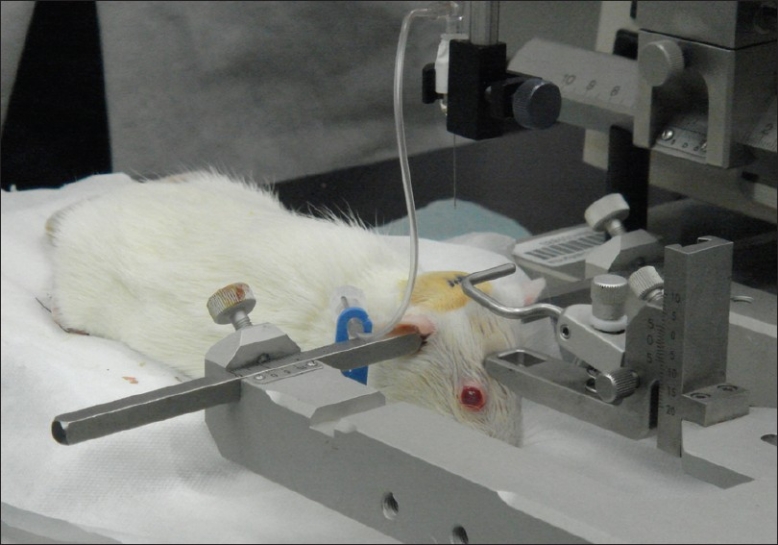
Rats are anesthetized and the ventral tail artery is exposed through a small (5 mm), midline incision, 0.2 mL of blood is taken from the artery and gentle pressure is applied for hemostasis. The rat is flipped prone, and with the head flexed to 90 degrees in a stereotactic frame, a 27G angiocath is advanced in a vertical trajectory, level with the external auditory canals. Upon puncturing the atlanto-occipital membrane, the needle is slowly advanced and observed for cerebrospinal fluid (CSF). A syringe withdraws 0.1 mL of CSF and the blood is injected into the subarachnoid space. The procedure is repeated 24 hours later by re-opening the tail incision. At 8 days, the rats are euthanized and their brains harvested, sectioned, and incubated with triphenyltetrazolium chloride (TTC).
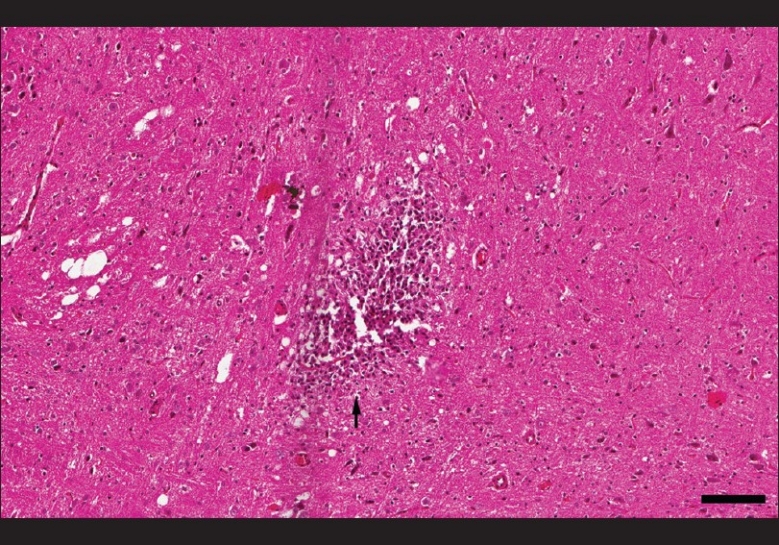
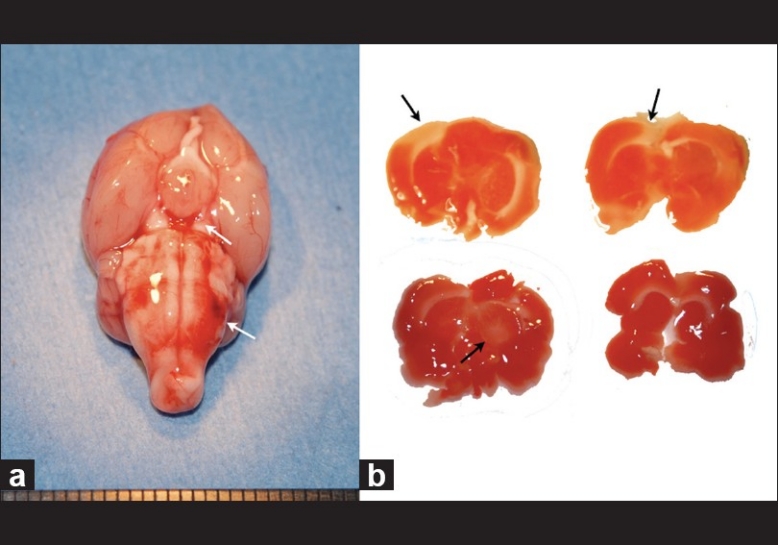
Rats develop neurological deficits consistent with vasospasm and infarction as previously described in double-injection models. Cortical and deep infarctions were demonstrated by TTC staining and on histopathology.
A minimally invasive, double-injection rat model of SAH and vasospasm is feasible and produces neurological deficits and infarction. This model can be used to study neuroprotective treatments for vasospasm and delayed neurological deficits following SAH, reducing the confounding effects of surgical interventions.
大鼠蛛网膜下腔出血(SAH)双注射模型在引发血管痉挛、延迟性神经功能缺损和梗死方面最为有效。然而,它们需要两次大型手术来暴露股动脉和寰枕膜。我们开发了一种微创改良方法,可防止手术操作的混杂效应、蛛网膜下腔出血以及将感染风险降至最低。
将大鼠麻醉,通过一个小的(5毫米)中线切口暴露腹侧尾动脉,从动脉中抽取0.2毫升血液,并施加轻柔压力止血。将大鼠翻转成俯卧位,在立体定位框架中将头部弯曲90度,沿垂直轨迹推进一根27G血管穿刺针,使其与外耳道处于同一水平。穿刺寰枕膜后,缓慢推进针头并观察脑脊液(CSF)。用注射器抽取0.1毫升脑脊液,然后将血液注入蛛网膜下腔。24小时后通过重新打开尾部切口重复该操作。在第8天,对大鼠实施安乐死并取出其大脑,进行切片,并用氯化三苯基四氮唑(TTC)孵育。
大鼠出现与双注射模型中先前描述的血管痉挛和梗死一致的神经功能缺损。TTC染色和组织病理学显示有皮质和深部梗死。
一种微创的SAH和血管痉挛双注射大鼠模型是可行的,并会产生神经功能缺损和梗死。该模型可用于研究SAH后血管痉挛和延迟性神经功能缺损的神经保护治疗,减少手术干预的混杂效应。