Department of Oncology, Skåne University Hospital, Lund, Sweden.
BMC Cancer. 2011 Aug 7;11:341. doi: 10.1186/1471-2407-11-341.
An increasing number of neo-adjuvant breast cancer studies are being conducted and a novel model for tumor biological studies, the "window-of-opportunity" model, has revealed several advantages. Change in tumor cell proliferation, estimated by Ki67-expression in pre-therapeutic core biopsies versus post-therapeutic surgical samples is often the primary end-point. The aim of the present study was to investigate potential differences in proliferation scores between core biopsies and surgical samples when patients have not received any intervening anti-cancer treatment. Also, a lack of consensus concerning Ki67 assessment may raise problems in the comparison of neo-adjuvant studies. Thus, the secondary aim was to present a novel model for Ki67 assessment.
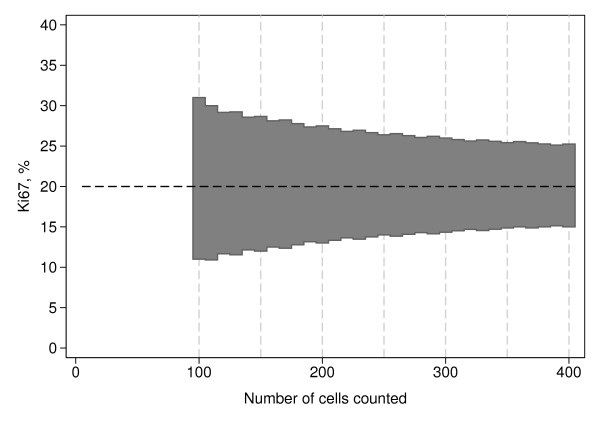
Fifty consecutive breast cancer cases with both a core biopsy and a surgical sample available, without intervening neo-adjuvant therapy, were collected and tumor proliferation (Ki67, MIB1 antibody) was assessed immunohistochemically. A theoretical model for the assessment of Ki67 was constructed based on sequential testing of the null hypothesis 20% Ki67-positive cells versus the two-sided alternative more or less than 20% positive cells..
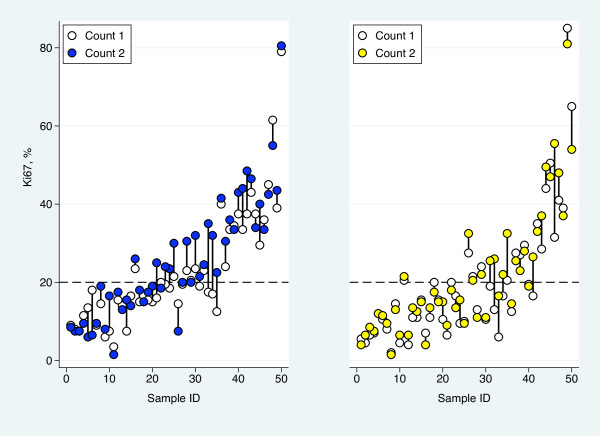
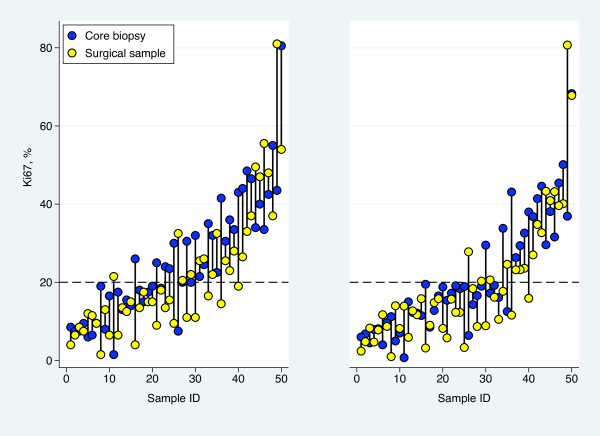
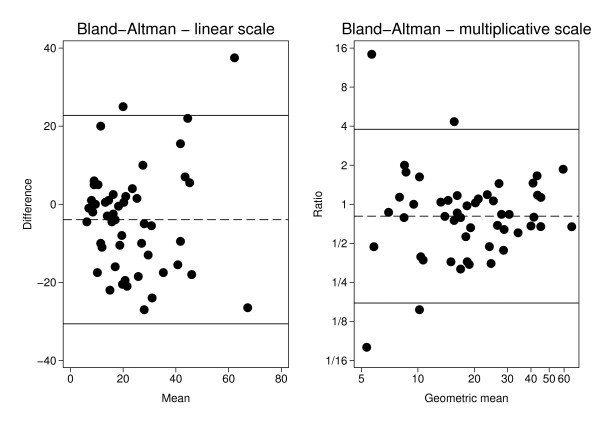
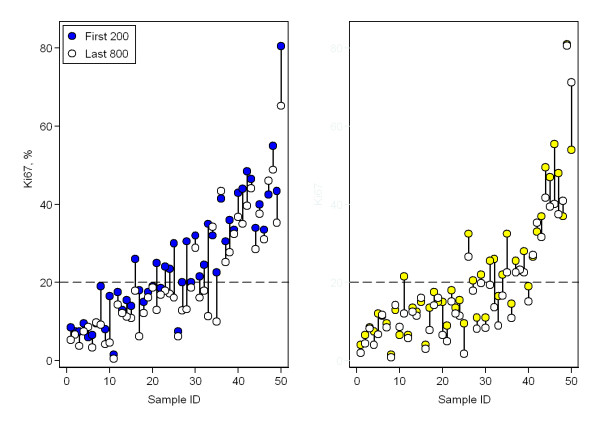
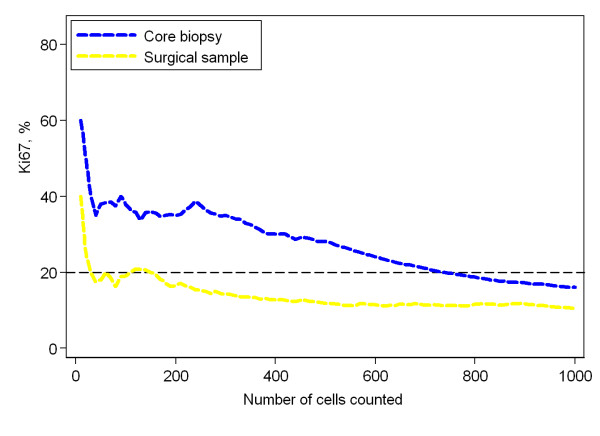
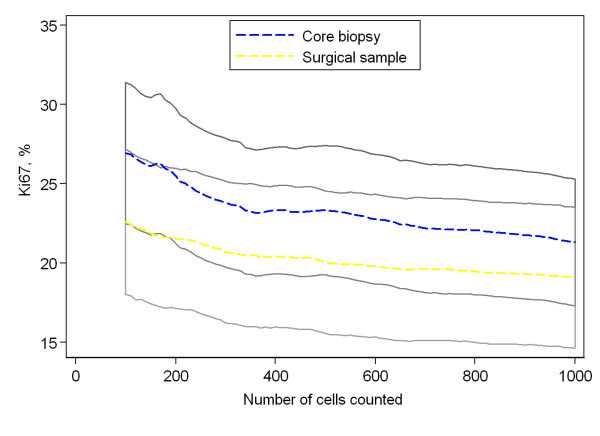
Assessment of Ki67 in 200 tumor cells showed an absolute average proliferation difference of 3.9% between core biopsies and surgical samples (p = 0.046, paired t-test) with the core biopsies being the more proliferative sample type. A corresponding analysis on the log-scale showed the average relative decrease from the biopsy to the surgical specimen to be 19% (p = 0.063, paired t-test on the log-scale). The difference was significant when using the more robust Wilcoxon matched-pairs signed-ranks test (p = 0.029). After dichotomization at 20%, 12 of the 50 sample pairs had discrepant proliferation status, 10 showed high Ki67 in the core biopsy compared to two in the surgical specimen (p = 0.039, McNemar's test). None of the corresponding results for 1000 tumor cells were significant - average absolute difference 2.2% and geometric mean of the ratios 0.85 (p = 0.19 and p = 0.18, respectively, paired t-tests, p = 0.057, Wilcoxon's test) and an equal number of discordant cases after dichotomization. Comparing proliferation values for the initial 200 versus the final 800 cancer cells showed significant absolute differences for both core biopsies and surgical samples 5.3% and 3.2%, respectively (p < 0.0001, paired t-test).
A significant difference between core biopsy and surgical sample proliferation values was observed despite no intervening therapy. Future neo-adjuvant breast cancer studies may have to take this into consideration.
越来越多的新辅助乳腺癌研究正在进行,一种新的肿瘤生物学研究模型,即“机会之窗”模型,已经显示出了一些优势。通过术前核心活检和术后手术样本中 Ki67 表达的变化来估计肿瘤细胞的增殖,这通常是主要终点。本研究的目的是调查在患者未接受任何干预性抗癌治疗的情况下,核心活检和手术样本之间增殖评分的潜在差异。此外,由于 Ki67 评估缺乏共识,可能会在新辅助研究的比较中产生问题。因此,次要目的是提出一种新的 Ki67 评估模型。
收集了 50 例连续的乳腺癌病例,这些病例均有核心活检和手术样本,且无新辅助治疗的介入。采用免疫组织化学方法检测肿瘤增殖(Ki67、MIB1 抗体)。根据 20%Ki67 阳性细胞与双侧替代假设的大于或小于 20%阳性细胞的零假设,构建了一种新的 Ki67 评估的理论模型。
在 200 个肿瘤细胞中评估 Ki67 时,核心活检和手术样本之间的绝对平均增殖差异为 3.9%(p = 0.046,配对 t 检验),核心活检样本增殖更为活跃。在对数尺度上的相应分析显示,从活检到手术标本的平均相对减少量为 19%(p = 0.063,对数尺度配对 t 检验)。当使用更稳健的 Wilcoxon 配对符号秩检验时,差异具有统计学意义(p = 0.029)。在 Ki67 为 20%的情况下进行二分类后,50 对样本中有 12 对增殖状态不一致,10 对核心活检中 Ki67 较高,而 2 对手术标本中 Ki67 较高(p = 0.039,McNemar 检验)。对于 1000 个肿瘤细胞的相应结果均无统计学意义,平均绝对差异为 2.2%,比值的几何平均值为 0.85(p = 0.19 和 p = 0.18,配对 t 检验,p = 0.057,Wilcoxon 检验),并且在二分类后,不一致的病例数相等。比较核心活检和手术样本中前 200 个和最后 800 个癌细胞的增殖值,在核心活检和手术样本中均观察到显著的绝对差异,分别为 5.3%和 3.2%(p < 0.0001,配对 t 检验)。
尽管没有介入治疗,但仍观察到核心活检和手术样本增殖值之间的显著差异。未来的新辅助乳腺癌研究可能需要考虑到这一点。