Department of Obstetrics and Gynecology, CTRC at UT Health Science Center, San Antonio, Texas 78229, USA.
Breast Cancer Res. 2011 Aug 11;13(3):R80. doi: 10.1186/bcr2929.
Current clinical strategies for treating hormonal breast cancer involve the use of anti-estrogens that block estrogen receptor (ER)α functions and aromatase inhibitors that decrease local and systemic estrogen production. Both of these strategies improve outcomes for ERα-positive breast cancer patients, however, development of therapy resistance remains a major clinical problem. Divergent molecular pathways have been described for this resistant phenotype and interestingly, the majority of downstream events in these resistance pathways converge upon the modulation of cell cycle regulatory proteins including aberrant activation of cyclin dependent kinase 2 (CDK2). In this study, we examined whether the CDK inhibitor roscovitine confers a tumor suppressive effect on therapy-resistant breast epithelial cells.
Using various in vitro and in vivo assays, we tested the effect of roscovitine on three hormonal therapy-resistant model cells: (a) MCF-7-TamR (acquired tamoxifen resistance model); (b) MCF-7-LTLTca (acquired letrozole resistance model); and (c) MCF-7-HER2 that exhibit tamoxifen resistance (ER-growth factor signaling cross talk model).
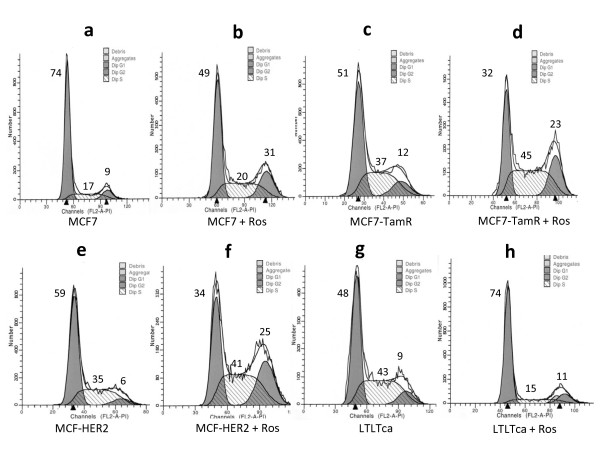
Hormonal therapy-resistant cells exhibited aberrant activation of the CDK2 pathway. Roscovitine at a dose of 20 μM significantly inhibited the cell proliferation rate and foci formation potential of all three therapy-resistant cells. The drug treatment substantially increased the proportion of cells in G2/M cell cycle phase with decreased CDK2 activity and promoted low cyclin D1 levels. Interestingly, roscovitine also preferentially down regulated the ERα isoform and ER-coregulators including AIB1 and PELP1. Results from xenograft studies further showed that roscovitine can attenuate growth of therapy-resistant tumors in vivo.
Roscovitine can reduce cell proliferation and survival of hormone therapy-resistant breast cancer cells. Our results support the emerging concept that inhibition of CDK2 activity has the potential to abrogate growth of hormonal therapy-resistant cells.
目前治疗激素型乳腺癌的临床策略包括使用抗雌激素药物来阻断雌激素受体(ER)α功能,以及使用芳香化酶抑制剂来减少局部和全身雌激素的产生。这两种策略都改善了 ERα阳性乳腺癌患者的预后,但治疗耐药性的发展仍然是一个主要的临床问题。已经描述了这种耐药表型的不同分子途径,有趣的是,这些耐药途径的大多数下游事件都集中在细胞周期调节蛋白的调节上,包括细胞周期蛋白依赖性激酶 2(CDK2)的异常激活。在这项研究中,我们研究了 CDK 抑制剂罗沙替丁乙酸酯是否对耐药性乳腺癌上皮细胞具有肿瘤抑制作用。
使用各种体外和体内测定,我们测试了罗沙替丁乙酸酯对三种激素治疗耐药模型细胞的影响:(a)MCF-7-TamR(获得性他莫昔芬耐药模型);(b)MCF-7-LTLTca(获得性来曲唑耐药模型);和(c)MCF-7-HER2,表现出他莫昔芬耐药(ER-生长因子信号交叉谈话模型)。
激素治疗耐药细胞表现出 CDK2 途径的异常激活。罗沙替丁乙酸酯在 20 μM 的剂量下显著抑制了所有三种耐药细胞的细胞增殖率和焦点形成潜力。药物治疗显著增加了细胞周期 G2/M 期的比例,降低了 CDK2 活性,并促进了低 cyclin D1 水平。有趣的是,罗沙替丁乙酸酯还优先下调了 ERα 同工型和 ER 共调节剂,包括 AIB1 和 PELP1。异种移植研究的结果进一步表明,罗沙替丁乙酸酯可以减少体内耐药肿瘤的生长。
罗沙替丁乙酸酯可以减少激素治疗耐药乳腺癌细胞的增殖和存活。我们的结果支持这样一种新兴的概念,即抑制 CDK2 活性有可能消除激素治疗耐药细胞的生长。