Department of International Health, Immunology and Microbiology, Faculty of Health Sciences, University of Copenhagen, Øster Farimagsgade 5, DK 1014 Copenhagen K, Denmark.
Malar J. 2011 Aug 15;10:238. doi: 10.1186/1475-2875-10-238.
Artemether-lumefantrine (ALu) replaced sulphadoxine-pymimethamine (SP) as the official first-line anti-malarial in Tanzania in November 2006. So far, artemisinin combination therapy (ACT) is contra-indicated during pregnancy by the national malaria treatment guidelines, and pregnant women depend on SP for Intermittent Preventive Treatment (IPTp) during pregnancy. SP is still being dispensed by private drug stores, but it is unknown to which extent. If significant, it may undermine its official use for IPTp through induction of resistance. The main study objective was to perform a baseline study of the private market for anti-malarials in Muheza town, an area with widespread anti-malarial drug resistance, prior to the implementation of a provider training and accreditation programme that will allow accredited drug shops to sell subsidized ALu.
All drug shops selling prescription-only anti-malarials, in Muheza town, Tanga Region voluntarily participated from July to December 2009. Qualitative in-depth interviews were conducted with owners or shopkeepers on saleability of anti-malarials, and structured questionnaires provided quantitative data on drugs sales volume.
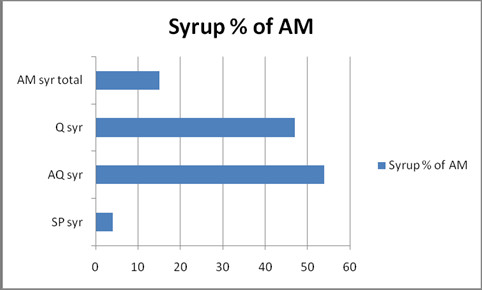
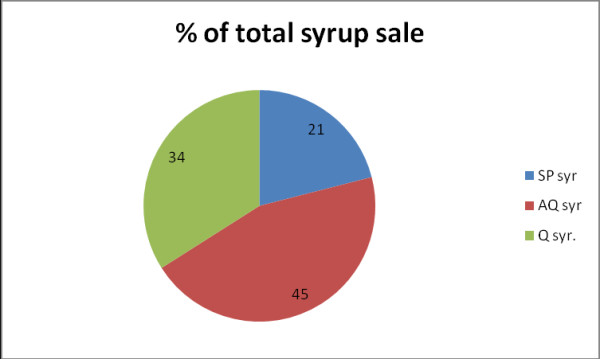
All surveyed drug shops illicitly sold SP and quinine (QN), and legally amodiaquine (AQ). Calculated monthly sale was 4,041 doses, in a town with a population of 15,000 people. Local brands of SP accounted for 74% of sales volume, compared to AQ (13%), QN (11%) and ACT (2%).
In community practice, the saleability of ACT was negligible. SP was best-selling, and use was not reserved for IPTp, as stipulated in the national anti-malarial policy. It is a major reason for concern that such drug-pressure in the community equals de facto intermittent presumptive treatment. In an area where SP drug resistance remains high, unregulated SP dispensing to people other than pregnant women runs the risk of eventually jeopardizing the effectiveness of the IPTp strategy. Further studies are recommended to find out barriers for ACT utilization and preference for self-medication and to train private drug dispensers.
青蒿琥酯-咯萘啶(ALu)于 2006 年 11 月取代磺胺多辛-乙胺嘧啶(SP)成为坦桑尼亚的官方一线抗疟药物。到目前为止,国家疟疾治疗指南规定在怀孕期间禁忌使用青蒿素类复方疗法(ACT),孕妇在怀孕期间依赖 SP 进行间歇性预防治疗(IPTp)。SP 仍在私人药店出售,但尚不清楚其具体数量。如果数量较大,可能会通过诱导耐药性而破坏其用于 IPTp 的官方用途。主要研究目的是在实施供应商培训和认证计划之前,对 Muheza 镇的私人抗疟药物市场进行基线研究,该计划将允许认证后的药店销售补贴后的 ALu。
2009 年 7 月至 12 月,坦噶地区 Muheza 镇所有销售处方抗疟药物的药店均自愿参与。对店主或店员进行了关于抗疟药物销售情况的定性深入访谈,并提供了关于药物销售量的结构化问卷提供了定量数据。
所有接受调查的药店均非法销售 SP 和奎宁(QN),以及合法的阿莫地喹(AQ)。在一个拥有 15000 人口的城镇中,每月销售量为 4041 剂。SP 的当地品牌占销售量的 74%,而 AQ(13%)、QN(11%)和 ACT(2%)。
在社区实践中,ACT 的销售情况微不足道。SP 是最畅销的药物,而且其使用并不限于国家抗疟政策规定的 IPTp。令人担忧的是,社区中存在如此大的药物压力,相当于事实上的间歇性推测性治疗。在 SP 耐药性仍然很高的地区,不受监管的 SP 向孕妇以外的人配药,有可能最终危及 IPTp 策略的有效性。建议进行进一步研究,以了解 ACT 利用的障碍以及自我用药的偏好,并对私人药物配药者进行培训。