Empilweni Services and Research Unit, Department of Paediatrics and Child Health, Rahima Moosa Mother and Child Hospital, University of the Witwatersrand Johannesburg, South Africa.
J Int AIDS Soc. 2011 Aug 15;14:42. doi: 10.1186/1758-2652-14-42.
Use of highly active antiretroviral therapy (HAART), a triple-drug combination, in HIV-infected pregnant women markedly reduces mother to child transmission of HIV and decreases maternal morbidity. However, there remains uncertainty about the effects of in utero exposure to HAART on foetal development.
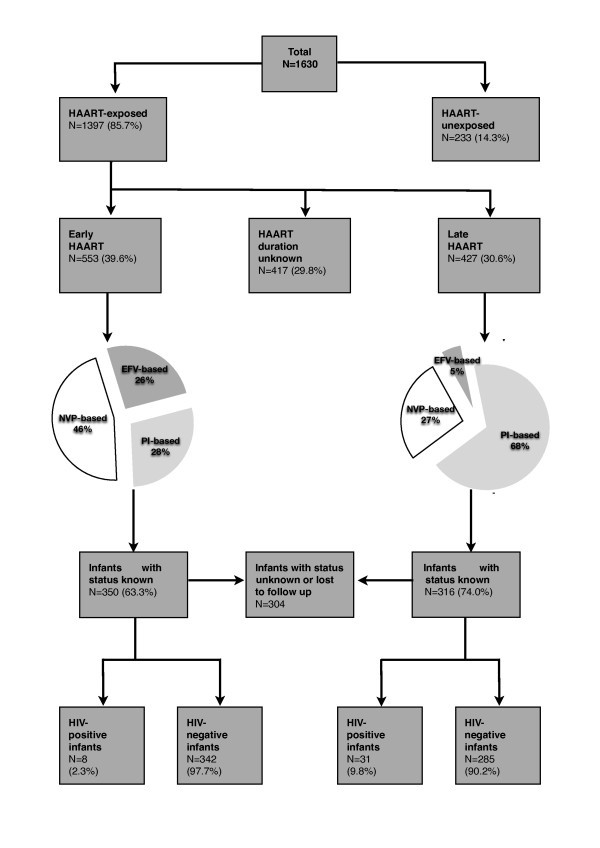
Our objectives were to investigate whether in utero exposure to HAART is associated with low birth weight and/or preterm birth in a population of South African women with advanced HIV disease. A retrospective observational study was performed on women with CD4 counts ≤250 cells/mm3 attending antenatal antiretroviral clinics in Johannesburg between October 2004 and March 2007. Low birth weight (<2.5 kg) and preterm birth rates (<37 weeks) were compared between those exposed and unexposed to HAART during pregnancy. Effects of different HAART regimen and duration were assessed.
Among HAART-unexposed infants, 27% (60/224) were low birth weight compared with 23% (90/388) of early HAART-exposed (exposed <28 weeks gestation) and 19% (76/407) of late HAART-exposed (exposed ≥28 weeks) infants (p = 0.05). In the early HAART group, a higher CD4 cell count was protective against low birth weight (AOR 0.57 per 50 cells/mm3 increase, 95% CI 0.45-0.71, p < 0.001) and preterm birth (AOR 0.68 per 50 cells/mm3 increase, 95% CI 0.55-0.85, p = 0.001). HAART exposure was associated with an increased preterm birth rate (15%, or 138 of 946, versus 5%, or seven of 147, in unexposed infants, p = 0.001), with early nevirapine and efavirenz-based regimens having the strongest associations with preterm birth (AOR 5.4, 95% CI 2.1-13.7, p < 0.001, and AOR 5.6, 95% CI 2.1-15.2, p = 0.001, respectively).
In this immunocompromised cohort, in utero HAART exposure was not associated with low birth weight. An association between NNRTI-based HAART and preterm birth was detected, but residual confounding is plausible. More advanced immunosuppression was a risk factor for low birth weight and preterm birth, highlighting the importance of earlier HAART initiation in women to optimize maternal health and improve infant outcomes.
在感染 HIV 的孕妇中使用高效抗逆转录病毒疗法(HAART),即三联药物组合,可以显著降低母婴 HIV 传播,并降低产妇发病率。然而,人们对于 HAART 对胎儿发育的影响仍存在不确定性。
我们的目的是调查在南非患有晚期 HIV 疾病的女性中,HAART 的宫内暴露是否与低出生体重和/或早产有关。对 2004 年 10 月至 2007 年 3 月期间在约翰内斯堡接受产前抗逆转录病毒治疗的 CD4 计数≤250 个细胞/mm3 的女性进行了回顾性观察性研究。比较了暴露于和未暴露于 HAART 的孕妇中低出生体重(<2.5 公斤)和早产(<37 周)的发生率。评估了不同 HAART 方案和持续时间的影响。
在未暴露于 HAART 的婴儿中,27%(60/224)为低出生体重,而早期 HAART 暴露(暴露<28 周妊娠)的婴儿中为 23%(90/388),晚期 HAART 暴露(暴露≥28 周妊娠)的婴儿中为 19%(76/407)(p=0.05)。在早期 HAART 组中,CD4 细胞计数每增加 50 个细胞/mm3,低出生体重的保护作用呈下降趋势(AOR 0.57,95%CI 0.45-0.71,p<0.001)和早产(AOR 0.68,95%CI 0.55-0.85,p=0.001)。HAART 暴露与早产发生率增加有关(15%,946 例中有 138 例,而未暴露于 HAART 的婴儿中为 5%,147 例中有 7 例,p=0.001),早期使用奈韦拉平和依非韦伦为基础的方案与早产的相关性最强(AOR 5.4,95%CI 2.1-13.7,p<0.001 和 AOR 5.6,95%CI 2.1-15.2,p=0.001)。
在免疫抑制人群中,HAART 的宫内暴露与低出生体重无关。发现基于 NNRTI 的 HAART 与早产之间存在关联,但可能存在残余混杂。更严重的免疫抑制是低出生体重和早产的危险因素,这突出表明应尽早开始 HAART 治疗,以优化产妇健康并改善婴儿结局。