Cowdell Imogen, Beck Katharina, Portwood Clara, Sexton Harriet, Kumarendran Mary, Brandon Zoe, Kirtley Shona, Hemelaar Joris
National Perinatal Epidemiology Unit, Oxford Population Health, Nuffield Department of Population Health, University of Oxford, Richard Doll Building, Old Road Campus, Oxford OX3 7LF, UK.
Centre for Statistics in Medicine, Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, University of Oxford, Oxford, UK.
EClinicalMedicine. 2022 Apr 6;46:101368. doi: 10.1016/j.eclinm.2022.101368. eCollection 2022 Apr.
The World Health Organization recommends protease inhibitor (PI)-based antiretroviral therapy (ART) as second-line and third-line regimens in pregnant women living with HIV (WLHIV). US, European, and UK guidelines include PI-based ART as first-line regimens, but advise against the use of lopinavir/ritonavir (LPV/r)-based ART, citing an increased risk of preterm birth (PTB). We aimed to assess the risk of adverse perinatal outcomes in WLHIV receiving PI-ART and the comparative risks associated with different PI-ART regimens.
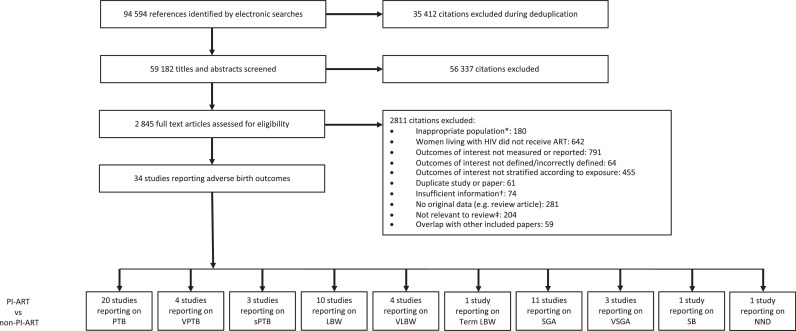
We conducted a systematic literature review by searching PubMed, CINAHL, Global Health, and EMBASE for studies published between Jan 1, 1980, and April 20, 2020. Two investigators independently selected studies and extracted data from studies reporting on the association of pregnant WLHIV receiving PI-ART with 11 perinatal outcomes: PTB, very PTB (VPTB), spontaneous PTB (sPTB), low birth weight (LBW), very LBW (VLBW), term LBW, preterm LBW, small for gestational age (SGA), very SGA (VSGA), stillbirth, and neonatal death. Pairwise random-effects meta-analyses examined the risk of each adverse perinatal outcome in WLHIV receiving PI-ART compared to non-PI-based ART (non-PI-ART), and comparisons of different PI-ART regimens. Quality assessments of studies were performed, subgroup and sensitivity analyses were conducted based on country income status and study quality, heterogeneity assessed, and the effect of adjustment for confounding factors assessed. The protocol is registered with PROSPERO, CRD42021248987.
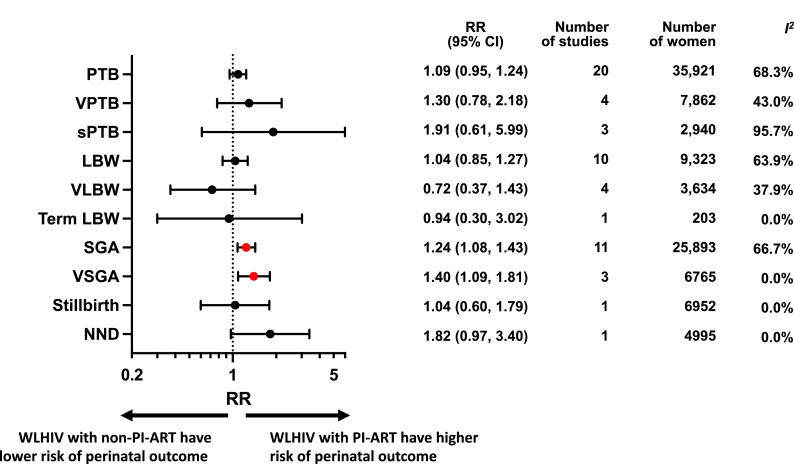
Of 94,594 studies identified, 34 cohort studies including 57,546 women met the inclusion criteria. Random-effects meta-analyses showed that PI-ART was associated with a significantly increased risk of SGA (Relative Risk [RR] 1.24, 95% CI 1.08-1.43; =66.7%) and VSGA (RR 1.40, 1.09-1.81; =0.0%), but not PTB (RR 1.09, 0.95-1.24; =68.3%), VPTB (RR 1.30, 0.78-2.18; =43.0%), sPTB (RR 1.91, 0.61-5.99; =95.7%), LBW (RR 1.04, 0.85-1.27; =63.9%), VLBW (RR 0.72, 0.37-1.43; =37.9%), term LBW (RR 0.94, 0.30-3.02; =0.0%), stillbirth (RR 1.04, 0.60-1.79; =0.0%), and neonatal death (RR 1.82, 0.97-3.40; =0.0%), compared to non-PI-ART. We found no significant differences in perinatal outcomes between ART regimens containing LPV/r, atazanavir/ritonavir (ATV/r), and darunavir/ritonavir (DRV/r), which are the most commonly used PIs.
PI-ART is associated with an increased risk of SGA and VSGA, but not PTB or other perinatal outcomes. No significant differences in perinatal outcomes were found between LPV/r, ATV/r, and DRV/r. These findings should inform clinical guidelines, and further efforts should be made to improve perinatal outcomes among pregnant WLHIV.
None.
世界卫生组织推荐以蛋白酶抑制剂(PI)为基础的抗逆转录病毒疗法(ART)作为感染HIV的孕妇(WLHIV)的二线和三线治疗方案。美国、欧洲和英国的指南将基于PI的ART作为一线治疗方案,但鉴于早产(PTB)风险增加,不建议使用基于洛匹那韦/利托那韦(LPV/r)的ART。我们旨在评估接受PI-ART的WLHIV发生不良围产期结局的风险,以及不同PI-ART方案相关的比较风险。
我们通过检索PubMed、CINAHL、Global Health和EMBASE,对1980年1月1日至2020年4月20日发表的研究进行了系统的文献综述。两名研究人员独立选择研究,并从报告接受PI-ART的妊娠WLHIV与11种围产期结局关联的研究中提取数据:PTB、极早产(VPTB)、自发性PTB(sPTB)、低出生体重(LBW)、极低出生体重(VLBW)、足月LBW、早产LBW、小于胎龄儿(SGA)、极小于胎龄儿(VSGA)、死产和新生儿死亡。成对随机效应荟萃分析检查了接受PI-ART的WLHIV与非基于PI的ART(非PI-ART)相比,每种不良围产期结局的风险,以及不同PI-ART方案的比较。对研究进行质量评估,根据国家收入状况和研究质量进行亚组和敏感性分析,评估异质性,并评估混杂因素调整的效果。该方案已在PROSPERO注册,注册号为CRD42021248987。
在识别出的94,594项研究中,34项队列研究(包括57,546名女性)符合纳入标准。随机效应荟萃分析表明,与非PI-ART相比,PI-ART与SGA(相对风险[RR]1.24,95%CI 1.08-1.43;I²=66.7%)和VSGA(RR 1.40,1.09-1.81;I²=0.0%)风险显著增加相关,但与PTB(RR 1.09,0.95-1.24;I²=68.3%)、VPTB(RR 1.30,0.78-2.18;I²=43.0%)、sPTB(RR 1.91,0.61-5.99;I²=95.7%)、LBW(RR 1.04,0.85-1.27;I²=63.9%)、VLBW(RR 0.72,0.37-1.43;I²=37.9%)、足月LBW(RR 0.94,0.30-3.02;I²=0.0%)、死产(RR 1.04,0.60-1.79;I²=0.0%)和新生儿死亡(RR 1.82,0.97-3.40;I²=0.0%)无关。我们发现,在最常用的PI(即LPV/r、阿扎那韦/利托那韦[ATV/r]和达芦那韦/利托那韦[DRV/r])的ART方案之间,围产期结局没有显著差异。
PI-ART与SGA和VSGA风险增加相关,但与PTB或其他围产期结局无关。在LPV/r、ATV/r和DRV/r之间,围产期结局没有显著差异。这些发现应为临床指南提供参考,应进一步努力改善妊娠WLHIV的围产期结局。
无。