Department of Social Medicine, University of Bristol, Bristol, United Kingdom.
PLoS One. 2011;6(8):e22309. doi: 10.1371/journal.pone.0022309. Epub 2011 Aug 11.
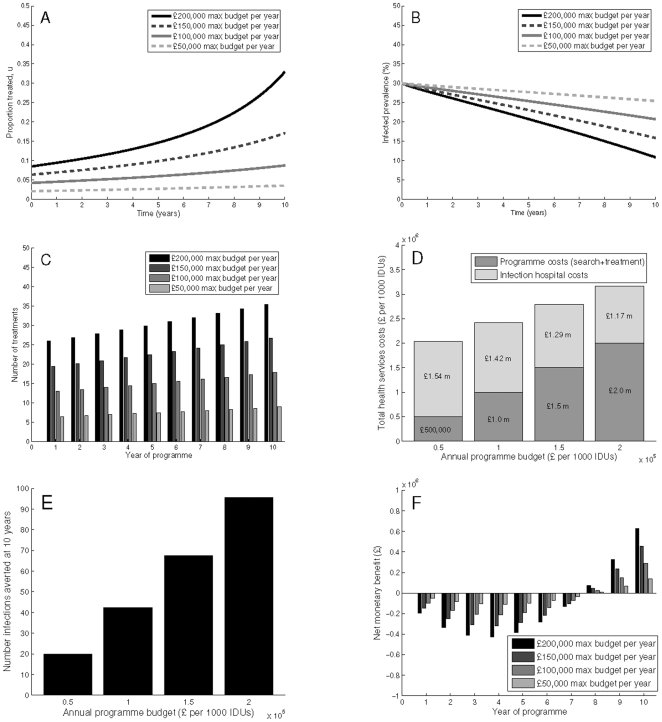
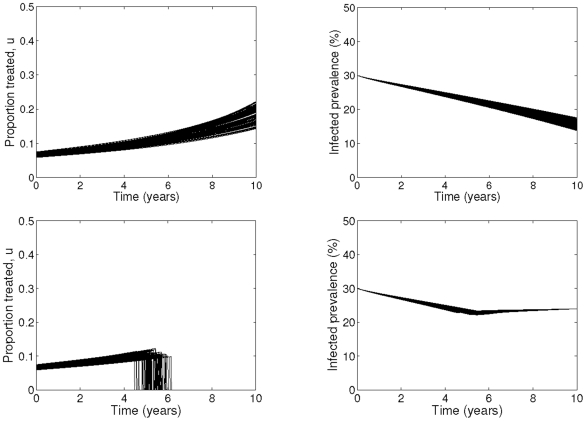
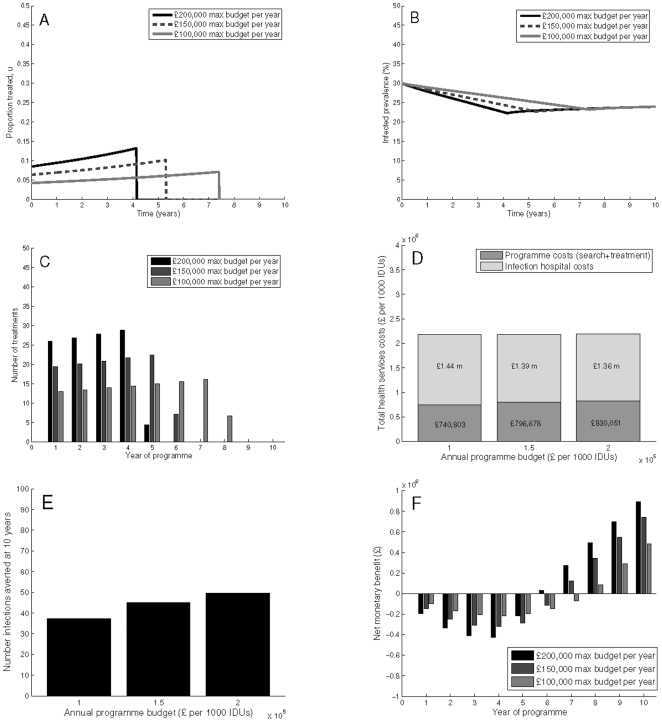
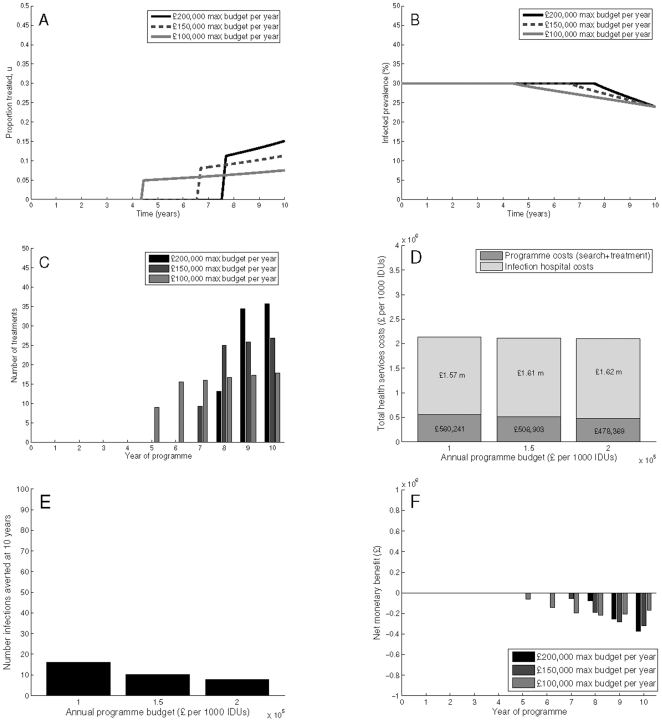
In most developed countries, HCV is primarily transmitted by injecting drug users (IDUs). HCV antiviral treatment is effective, and deemed cost-effective for those with no re-infection risk. However, few active IDUs are currently treated. Previous modelling studies have shown antiviral treatment for active IDUs could reduce HCV prevalence, and there is emerging interest in developing targeted IDU treatment programmes. However, the optimal timing and scale-up of treatment is unknown, given the real-world constraints commonly existing for health programmes. We explore how the optimal programme is affected by a variety of policy objectives, budget constraints, and prevalence settings. We develop a model of HCV transmission and treatment amongst active IDUs, determine the optimal treatment programme strategy over 10 years for two baseline chronic HCV prevalence scenarios (30% and 45%), a range of maximum annual budgets (£50,000-300,000 per 1,000 IDUs), and a variety of objectives: minimising health service costs and health utility losses; minimising prevalence at 10 years; minimising health service costs and health utility losses with a final time prevalence target; minimising health service costs with a final time prevalence target but neglecting health utility losses. The largest programme allowed for a given budget is the programme which minimises both prevalence at 10 years, and HCV health utility loss and heath service costs, with higher budgets resulting in greater cost-effectiveness (measured by cost per QALY gained compared to no treatment). However, if the objective is to achieve a 20% relative prevalence reduction at 10 years, while minimising both health service costs and losses in health utility, the optimal treatment strategy is an immediate expansion of coverage over 5-8 years, and is less cost-effective. By contrast, if the objective is only to minimise costs to the health service while attaining the 20% prevalence reduction, the programme is deferred until the final years of the decade, and is the least cost-effective of the scenarios.
在大多数发达国家,丙型肝炎病毒(HCV)主要通过注射吸毒者(IDUs)传播。HCV 抗病毒治疗有效,并且对于没有再次感染风险的人来说是具有成本效益的。然而,目前只有少数活跃的 IDUs 接受治疗。以前的建模研究表明,对活跃的 IDUs 进行抗病毒治疗可以降低 HCV 的流行率,并且人们对开发针对 IDU 的治疗方案越来越感兴趣。然而,鉴于卫生计划中通常存在的现实限制,尚不清楚最佳治疗时机和扩大治疗范围。我们探讨了各种政策目标、预算限制和流行率设定如何影响最佳方案。我们开发了一个 HCV 在活跃 IDUs 中传播和治疗的模型,为两种基线慢性 HCV 流行率情况(30%和 45%)确定了 10 年内最佳治疗方案策略,一个范围的最高年度预算(每位 IDU 每年 50,000 至 300,000 英镑),以及各种目标:最大限度地降低卫生服务成本和健康效用损失;在 10 年内最大限度地降低流行率;在最终时间流行率目标下,最大限度地降低卫生服务成本和健康效用损失;在最终时间流行率目标下,最大限度地降低卫生服务成本,但忽略健康效用损失。在给定预算下允许的最大方案是在 10 年内同时最小化流行率、HCV 健康效用损失和卫生服务成本的方案,较高的预算会带来更高的成本效益(通过与不治疗相比,每获得一个 QALY 的成本来衡量)。然而,如果目标是在 10 年内将相对流行率降低 20%,同时最小化卫生服务成本和健康效用损失,那么最佳治疗策略是在 5-8 年内立即扩大覆盖范围,并且成本效益较低。相比之下,如果目标只是在达到 20%的流行率降低的同时,最大限度地降低卫生服务成本,那么该方案将推迟到该十年的最后几年,并且是所有方案中成本效益最低的。