Service de Médecine Physique et de Réadaptation, CHU R.Poincaré, Garches, France.
PLoS One. 2011;6(8):e23129. doi: 10.1371/journal.pone.0023129. Epub 2011 Aug 10.
The preoperative Heterotopic Ossification (HO) extent is usually one of the main used criteria to predict the recurrence before excision. Brooker et al built a radiologic scale to assess this pre operative extent around the hip. The aim of this study is to investigate the relationship between the recurrence risk after hip HO excision in Traumatic Brain Injury (TBI) and Spinal Cord Injury (SCI) patients and the preoperative extent of HO.
METHODOLOGY/PRINCIPAL FINDINGS: A case control study including TBI or SCI patients following surgery for troublesome hip HO with (case, n = 19) or without (control, n = 76) recurrence. Matching criteria were: sex, pathology (SCI or TBI) and age at the time of surgery (+/-4.5 years). For each etiology (TBI and SCI), the residual cognitive and functional status (Garland classification), the preoperative extent (Brooker status), the modified radiological and functional status (GCG-BD classification), HO localization, side, mean age at the CNS damage, mean delay for the first HO surgery, and for the case series, the mean operative delay for recurrence after the first surgical intervention were noted.
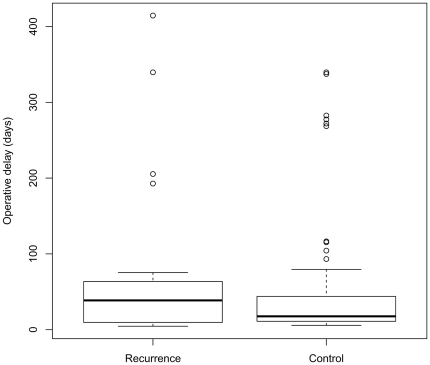
CONCLUSIONS/SIGNIFICANCE: The median delay for first HO surgery was 38.6 months (range 4.5 to 414.5;) for the case subgroup and 17.6 months (range 5.7 to 339.6) for the control group. No significant link was found between recurrence and operative delay (p = 0.51); the location around the joint (0.07); the Brooker (p = 0.52) or GCG-BD status (p = 0.79). Including all the matching factors, no significant relationship was found between the recurrence HO risk and the preoperative extent of troublesome hip HO using Brooker status (OR = 1.56(95% CI: 0.47-5.19)) or GCG-BD status (OR class 3 versus 2 = 0.67(95% CI: 0.11-4.24) and OR class 4 versus 2 = 0.79(95%CI: 0.09-6.91)). Until the pathophysiology of HO development is understood, it will be difficult to create tools which can predict HO recurrence.
术前异位骨化(HO)的程度通常是切除前预测复发的主要标准之一。布鲁克等人建立了一种放射学量表来评估髋关节周围的术前范围。本研究的目的是探讨创伤性脑损伤(TBI)和脊髓损伤(SCI)患者髋关节 HO 切除术后复发风险与 HO 术前程度的关系。
方法/主要发现:一项病例对照研究,纳入了因髋关节 HO 而接受手术治疗的 TBI 或 SCI 患者(病例组,n=19)或无复发的患者(对照组,n=76)。匹配标准为:性别、病理学(SCI 或 TBI)和手术时的年龄(+/-4.5 岁)。对于每种病因(TBI 和 SCI),记录残留的认知和功能状态(加兰德分类)、术前程度(布鲁克状态)、改良放射学和功能状态(GCG-BD 分类)、HO 定位、侧别、中枢神经系统损伤时的平均年龄、第一次 HO 手术的平均延迟时间,以及对于病例系列,第一次手术干预后复发的平均手术延迟时间。
结论/意义:病例亚组的第一次 HO 手术中位延迟时间为 38.6 个月(范围 4.5 至 414.5),对照组为 17.6 个月(范围 5.7 至 339.6)。复发与手术延迟之间无显著关联(p=0.51);关节周围的位置(0.07);布鲁克(p=0.52)或 GCG-BD 状态(p=0.79)。包括所有匹配因素在内,使用布鲁克状态(OR=1.56(95%CI:0.47-5.19))或 GCG-BD 状态(OR 3 级与 2 级=0.67(95%CI:0.11-4.24)和 OR 4 级与 2 级=0.79(95%CI:0.09-6.91)),髋关节 HO 切除术后复发的风险与术前髋关节 HO 程度之间均无显著相关性。在了解 HO 发展的病理生理学之前,很难创建可以预测 HO 复发的工具。