Maine Medical Center Research Institute, 81 Research Drive, Scarborough, ME 04074, USA.
Bone. 2012 Feb;50(2):490-8. doi: 10.1016/j.bone.2011.08.005. Epub 2011 Aug 11.
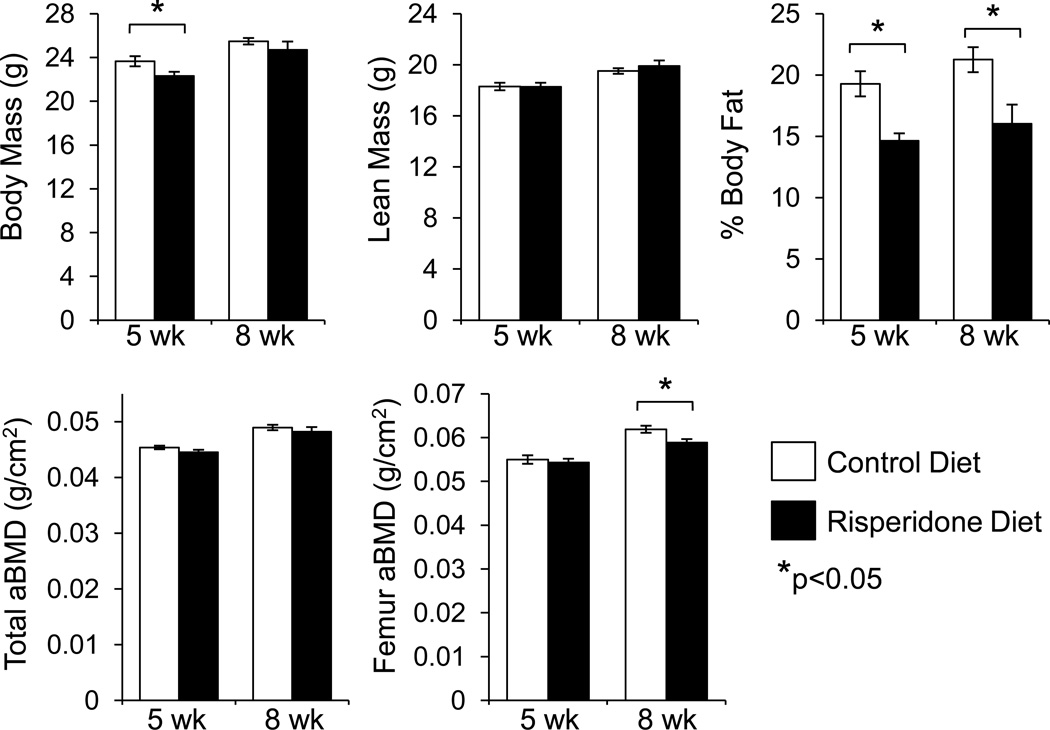
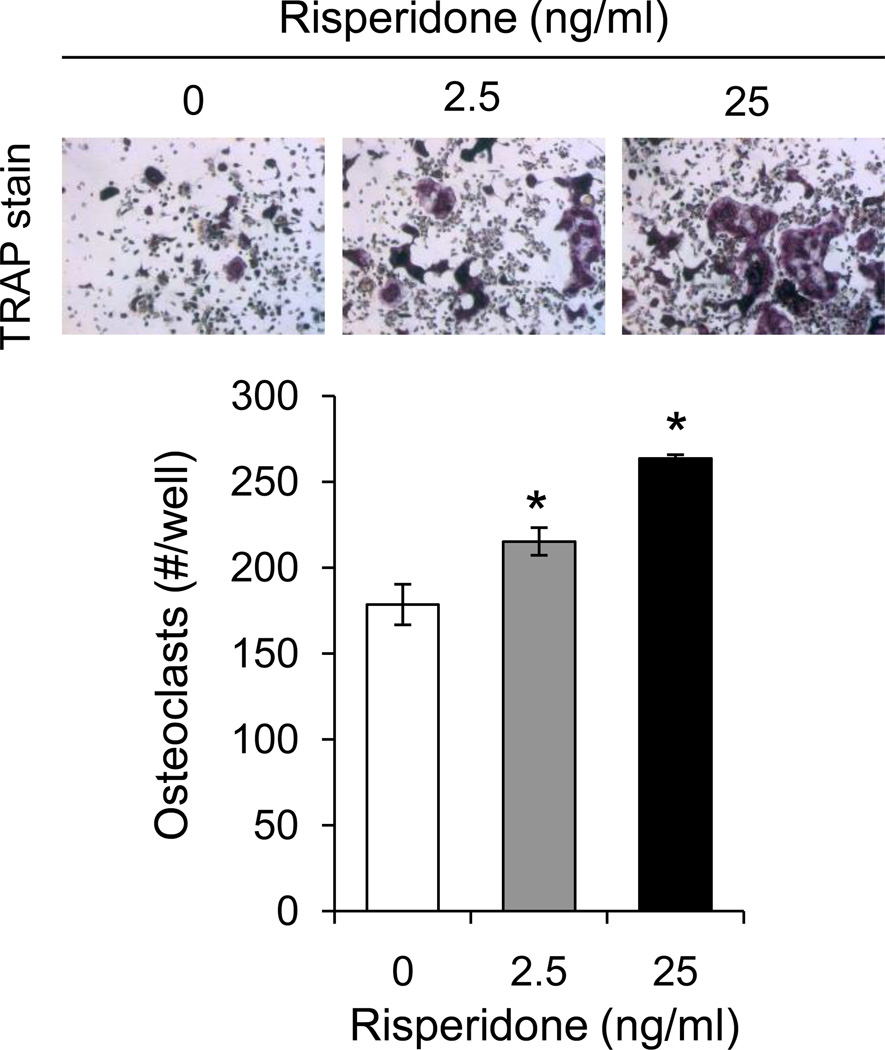
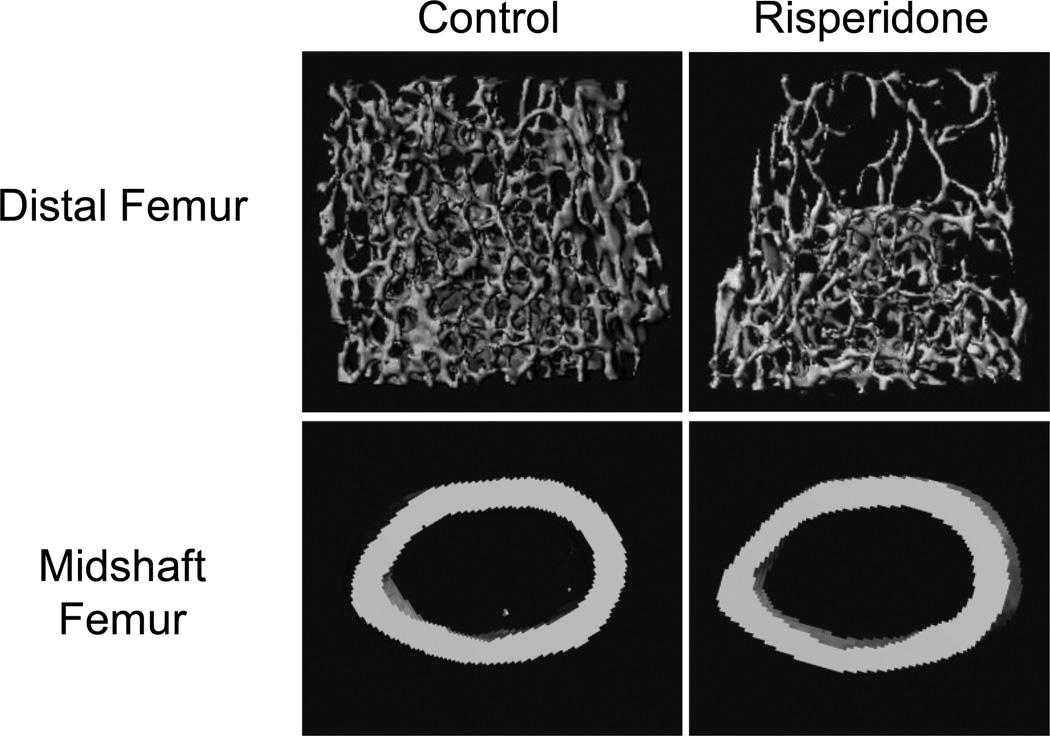
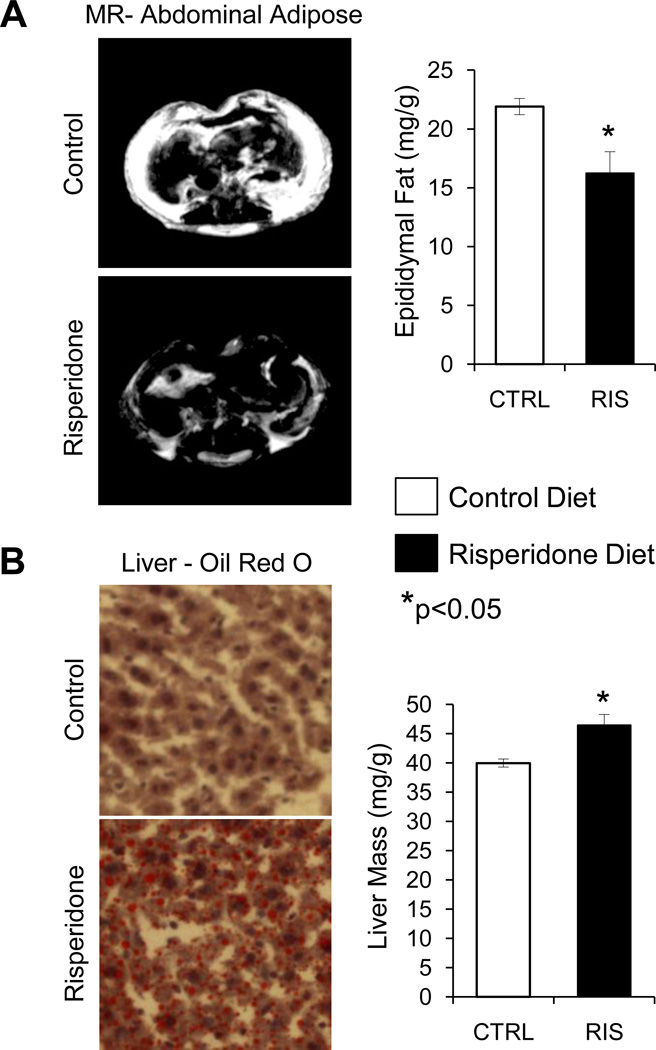
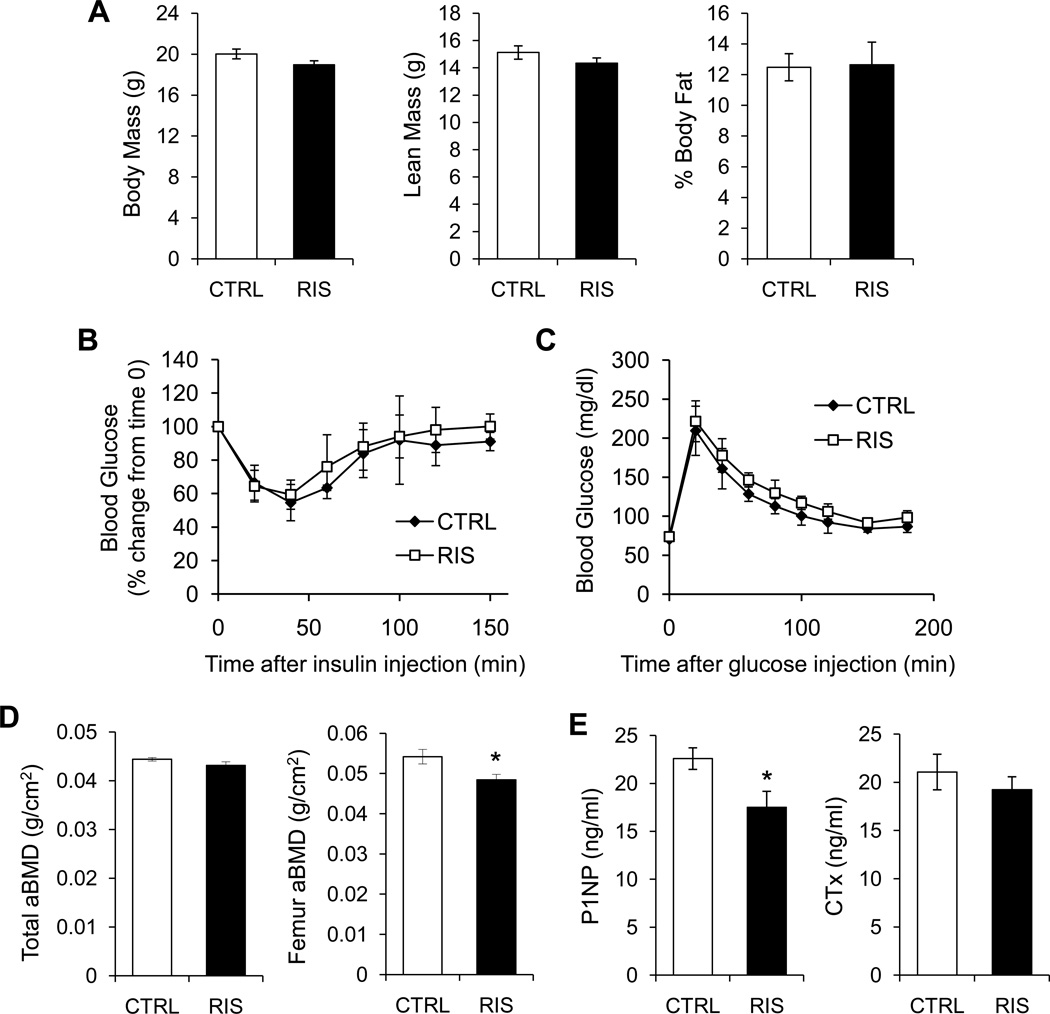
Second generation antipsychotics (SGAs) have been linked to metabolic and bone disorders in clinical studies, but the mechanisms of these side effects remain unclear. Additionally, no studies have examined whether SGAs cause bone loss in mice. Using in vivo and in vitro modeling we examined the effects of risperidone, the most commonly prescribed SGA, on bone in C57BL6/J (B6) mice. Mice were treated with risperidone orally by food supplementation at a dose of 1.25 mg/kg daily for 5 and 8 weeks, starting at 3.5 weeks of age. Risperidone reduced trabecular BV/TV, trabecular number and percent cortical area. Trabecular histomorphometry demonstrated increased resorption parameters, with no change in osteoblast number or function. Risperidone also altered adipose tissue distribution such that white adipose tissue mass was reduced and liver had significantly higher lipid infiltration. Next, in order to tightly control risperidone exposure, we administered risperidone by chronic subcutaneous infusion with osmotic minipumps (0.5 mg/kg daily for 4 weeks) in 7 week old female B6 mice. Similar trabecular and cortical bone differences were observed compared to the orally treated groups (reduced trabecular BV/TV, and connectivity density, and reduced percent cortical area) with no change in body mass, percent body fat, glucose tolerance or insulin sensitivity. Unlike in orally treated mice, risperidone infusion reduced bone formation parameters (serum P1NP, MAR and BFR/BV). Resorption parameters were elevated, but this increase did not reach statistical significance. To determine if risperidone could directly affect bone cells, primary bone marrow cells were cultured with osteoclast or osteoblast differentiation media. Risperidone was added to culture medium in clinically relevant doses of 0, 2.5 or 25 ng/ml. The number of osteoclasts was significantly increased by addition in vitro of risperidone while osteoblast differentiation was not altered. These studies indicate that risperidone treatment can have negative skeletal consequences by direct activation of osteoclast activity and by indirect non-cell autonomous mechanisms. Our findings further support the tenet that the negative side effects of SGAs on bone mass should be considered when weighing potential risks and benefits, especially in children and adolescents who have not yet reached peak bone mass.
第二代抗精神病药物(SGAs)在临床研究中与代谢和骨骼疾病有关,但这些副作用的机制仍不清楚。此外,尚无研究检查 SGA 是否会导致小鼠的骨质流失。使用体内和体外模型,我们研究了最常开的 SGA 利培酮对 C57BL6/J(B6)小鼠骨骼的影响。从 3.5 周龄开始,通过食物补充的方式,每天以 1.25mg/kg 的剂量给小鼠口服利培酮,连续治疗 5 和 8 周。利培酮降低了小梁骨 BV/TV、小梁数和皮质面积百分比。小梁组织形态计量学显示吸收参数增加,而成骨细胞数量或功能没有变化。利培酮还改变了脂肪组织的分布,使白色脂肪组织质量减少,肝脏脂质浸润显著增加。接下来,为了严格控制利培酮的暴露,我们通过慢性皮下输注渗透微型泵(每天 0.5mg/kg,持续 4 周)在 7 周龄雌性 B6 小鼠中给予利培酮。与口服治疗组相比,观察到类似的小梁和皮质骨差异(小梁骨 BV/TV 和连接密度降低,皮质面积百分比降低),体重、体脂百分比、葡萄糖耐量或胰岛素敏感性没有变化。与口服治疗的小鼠不同,利培酮输注降低了骨形成参数(血清 P1NP、MAR 和 BFR/BV)。吸收参数升高,但未达到统计学意义。为了确定利培酮是否可以直接影响骨细胞,我们将原代骨髓细胞与破骨细胞或成骨细胞分化培养基一起培养。将利培酮以临床相关剂量 0、2.5 或 25ng/ml 添加到培养基中。体外加入利培酮可显著增加破骨细胞的数量,而不改变成骨细胞的分化。这些研究表明,利培酮治疗可能通过直接激活破骨细胞活性和间接非细胞自主机制对骨骼产生负面影响。我们的研究结果进一步支持这样的观点,即在权衡潜在风险和益处时,应考虑 SGA 对骨量的负面影响,尤其是在尚未达到峰值骨量的儿童和青少年中。