Molina Rafael, Escudero Jose M, Augé Jose M, Filella Xavier, Foj Laura, Torné Aureli, Lejarcegui Jose, Pahisa Jaume
Laboratory of Clinical Biochemistry (Unit for Cancer Research), Hospital Clínic, Medical School, Barcelona, Spain.
Tumour Biol. 2011 Dec;32(6):1087-95. doi: 10.1007/s13277-011-0204-3. Epub 2011 Aug 24.
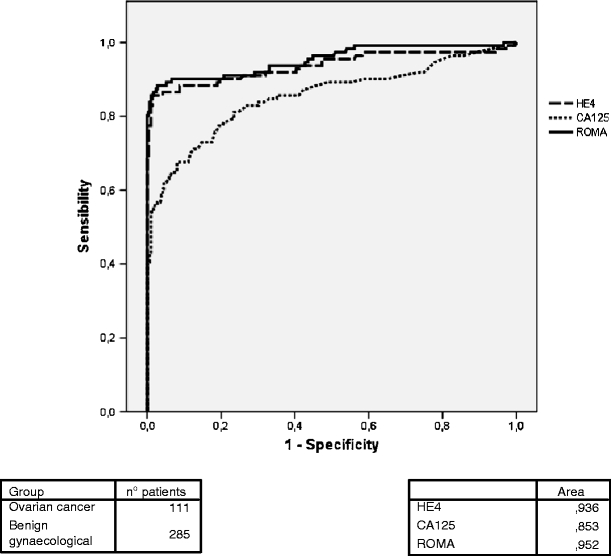
The aim of this study is to evaluate a new tumour marker, HE4, in comparison with CA 125 and the Risk of Ovarian Malignancy Algorithm (ROMA) in healthy women and in patients with benign and malignant gynaecological diseases. CA 125 and HE4 serum levels were determined in 66 healthy women, 285 patients with benign gynaecological diseases (68 endometriosis, 56 myomas, 137 ovarian cysts and 24 with other diseases), 33 patients with non-active gynaecological cancer and 143 with active gynaecological cancer (111 ovarian cancers). CA 125 and HE4 cut-offs were 35 U/mL and 150 pmol/L, respectively. ROMA algorithm cut-off was 13.1 and 27.7 for premenopausal or postmenopausal women, respectively. HE4, CA 125 and ROMA results were abnormal in 1.5%, 13.6% and 25.8% of healthy women and in 1.1%, 30.2% and 12.3% of patients with benign diseases, respectively. Among patients with cancer, HE4 (in contrast to CA 125) had significantly higher concentrations in ovarian cancer than in other malignancies (p < 0.001). Tumour marker sensitivity in ovarian cancer was 79.3% for HE4, 82.9% for CA 125 and 90.1% for ROMA. Both tumour markers, HE4 and CA 125 were related to tumour stage and histological type, with the lowest concentrations in mucinous tumours. A significantly higher area under the ROC curve was obtained with ROMA and HE4 than with CA 125 in the differential diagnosis of benign gynaecological diseases versus malignant ovarian cancer (0.952, 0.936 and 0.853, respectively). Data from our population indicate that ROMA algorithm might be further improved if it is used only in patients with normal HE4 and abnormal CA 125 serum levels (cancer risk for this profile is 44.4%). ROMA algorithm in HE4 positive had a similar sensitivity and only increases the specificity by 3.2% compared to HE4 alone.
本研究旨在评估一种新的肿瘤标志物HE4,并将其与CA 125以及卵巢恶性肿瘤风险算法(ROMA)在健康女性、患有良性和恶性妇科疾病的患者中进行比较。对66名健康女性、285名患有良性妇科疾病的患者(68例子宫内膜异位症、56例肌瘤、137例卵巢囊肿和24例患有其他疾病)、33例非活动性妇科癌症患者和143例活动性妇科癌症患者(111例卵巢癌)测定了CA 125和HE4血清水平。CA 125和HE4的临界值分别为35 U/mL和150 pmol/L。ROMA算法对于绝经前或绝经后女性的临界值分别为13.1和27.7。HE4、CA 125和ROMA结果在健康女性中的异常率分别为1.5%、13.6%和25.8%,在患有良性疾病的患者中的异常率分别为1.1%、30.2%和12.3%。在癌症患者中,HE4(与CA 125不同)在卵巢癌中的浓度显著高于其他恶性肿瘤(p < 0.001)。卵巢癌中HE4的肿瘤标志物敏感性为79.3%,CA 125为82.9%,ROMA为90.1%。HE4和CA 125这两种肿瘤标志物均与肿瘤分期和组织学类型相关,在黏液性肿瘤中的浓度最低。在鉴别诊断良性妇科疾病与恶性卵巢癌时,ROMA和HE4的ROC曲线下面积显著高于CA 125(分别为0.952、0.936和0.853)。我们人群的数据表明,如果仅在HE4正常而CA 125血清水平异常的患者中使用ROMA算法,可能会进一步改善(该特征的癌症风险为44.4%)。HE4阳性的ROMA算法具有相似的敏感性,与单独使用HE4相比,特异性仅提高3.2%。