Medicine Service, Denver Health and Department of Medicine, University of Colorado Denver Health Sciences Center, Denver, CO 80204-4507, USA.
N Engl J Med. 2011 Aug 25;365(8):689-98. doi: 10.1056/NEJMoa1104623.
Acute exacerbations adversely affect patients with chronic obstructive pulmonary disease (COPD). Macrolide antibiotics benefit patients with a variety of inflammatory airway diseases.
We performed a randomized trial to determine whether azithromycin decreased the frequency of exacerbations in participants with COPD who had an increased risk of exacerbations but no hearing impairment, resting tachycardia, or apparent risk of prolongation of the corrected QT interval.
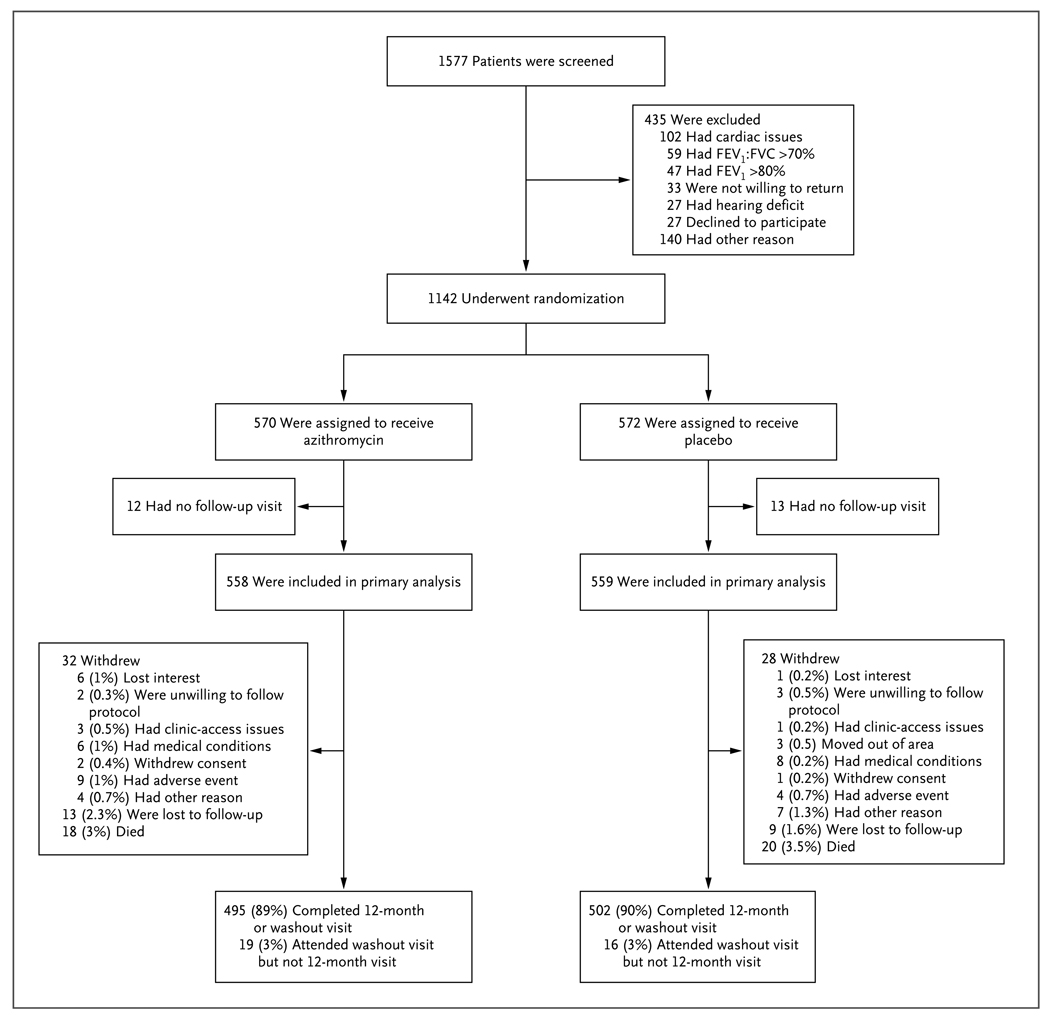
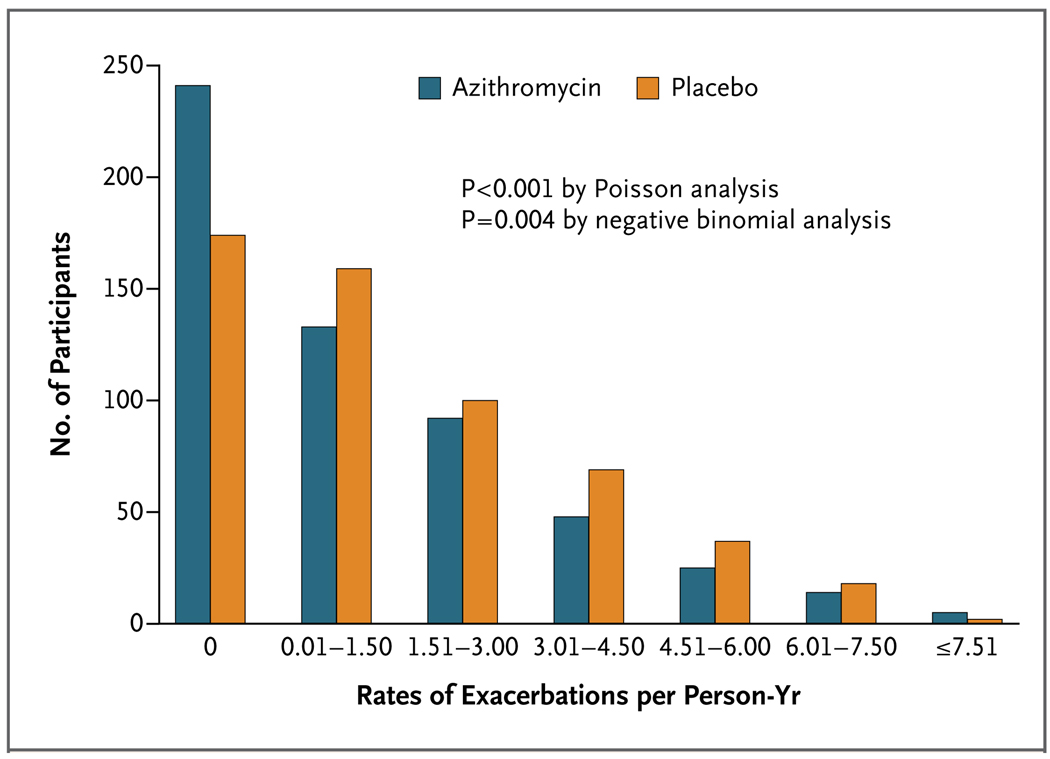
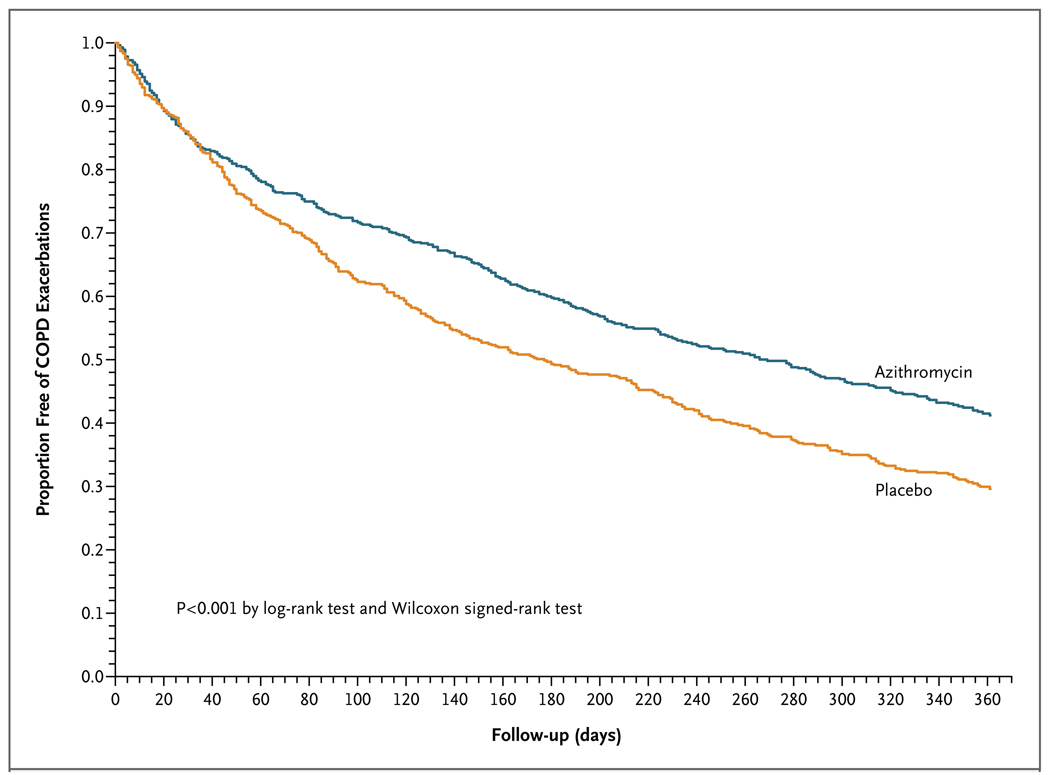
A total of 1577 subjects were screened; 1142 (72%) were randomly assigned to receive azithromycin, at a dose of 250 mg daily (570 participants), or placebo (572 participants) for 1 year in addition to their usual care. The rate of 1-year follow-up was 89% in the azithromycin group and 90% in the placebo group. The median time to the first exacerbation was 266 days (95% confidence interval [CI], 227 to 313) among participants receiving azithromycin, as compared with 174 days (95% CI, 143 to 215) among participants receiving placebo (P<0.001). The frequency of exacerbations was 1.48 exacerbations per patient-year in the azithromycin group, as compared with 1.83 per patient-year in the placebo group (P=0.01), and the hazard ratio for having an acute exacerbation of COPD per patient-year in the azithromycin group was 0.73 (95% CI, 0.63 to 0.84; P<0.001). The scores on the St. George's Respiratory Questionnaire (on a scale of 0 to 100, with lower scores indicating better functioning) improved more in the azithromycin group than in the placebo group (a mean [±SD] decrease of 2.8±12.8 vs. 0.6±11.4, P=0.004); the percentage of participants with more than the minimal clinically important difference of -4 units was 43% in the azithromycin group, as compared with 36% in the placebo group (P=0.03). Hearing decrements were more common in the azithromycin group than in the placebo group (25% vs. 20%, P=0.04).
Among selected subjects with COPD, azithromycin taken daily for 1 year, when added to usual treatment, decreased the frequency of exacerbations and improved quality of life but caused hearing decrements in a small percentage of subjects. Although this intervention could change microbial resistance patterns, the effect of this change is not known. (Funded by the National Institutes of Health; ClinicalTrials.gov number, NCT00325897.).
急性加重会对慢性阻塞性肺疾病(COPD)患者造成不良影响。大环内酯类抗生素对多种炎症性气道疾病患者有益。
我们进行了一项随机试验,以确定阿奇霉素是否会降低有加重风险但无听力损伤、静息心动过速或明显延长校正 QT 间期风险的 COPD 患者的加重频率。
共筛选了 1577 名受试者;1142 名(72%)随机接受阿奇霉素(每日 250mg,570 名参与者)或安慰剂(572 名参与者)治疗,为期 1 年,同时接受常规治疗。阿奇霉素组和安慰剂组的 1 年随访率分别为 89%和 90%。接受阿奇霉素治疗的参与者首次加重的中位时间为 266 天(95%置信区间 [CI],227 至 313),而接受安慰剂治疗的参与者为 174 天(95% CI,143 至 215)(P<0.001)。阿奇霉素组的加重频率为 1.48 次/患者-年,而安慰剂组为 1.83 次/患者-年(P=0.01),阿奇霉素组每患者-年 COPD 急性加重的风险比为 0.73(95% CI,0.63 至 0.84;P<0.001)。阿奇霉素组的圣乔治呼吸问卷(0 至 100 分,分数越低表示功能越好)评分改善程度大于安慰剂组(平均[±SD]下降 2.8±12.8 分 vs. 0.6±11.4 分,P=0.004);阿奇霉素组中超过最小临床重要差异-4 分的患者比例为 43%,而安慰剂组为 36%(P=0.03)。阿奇霉素组的听力下降发生率高于安慰剂组(25% vs. 20%,P=0.04)。
在选定的 COPD 患者中,阿奇霉素每日服用 1 年,联合常规治疗可降低加重频率并提高生活质量,但会导致一小部分患者出现听力下降。尽管这种干预可能会改变微生物耐药模式,但这种变化的影响尚不清楚。(由美国国立卫生研究院资助;临床试验.gov 编号,NCT00325897)。