Center for Healthful Behavior Change, Division of General Internal Medicine, Department of Medicine, New York University School of Medicine, 550 First Avenue, New York, NY, USA.
Implement Sci. 2011 Sep 1;6:100. doi: 10.1186/1748-5908-6-100.
Effectiveness of combined physician and patient-level interventions for blood pressure (BP) control in low-income, hypertensive African Americans with multiple co-morbid conditions remains largely untested in community-based primary care practices. Demographic, clinical, psychosocial, and behavioral characteristics of participants in the Counseling African American to Control Hypertension (CAATCH) Trial are described. CAATCH evaluates the effectiveness of a multi-level, multi-component, evidence-based intervention compared with usual care (UC) in improving BP control among poorly controlled hypertensive African Americans who receive primary care in Community Health Centers (CHCs).
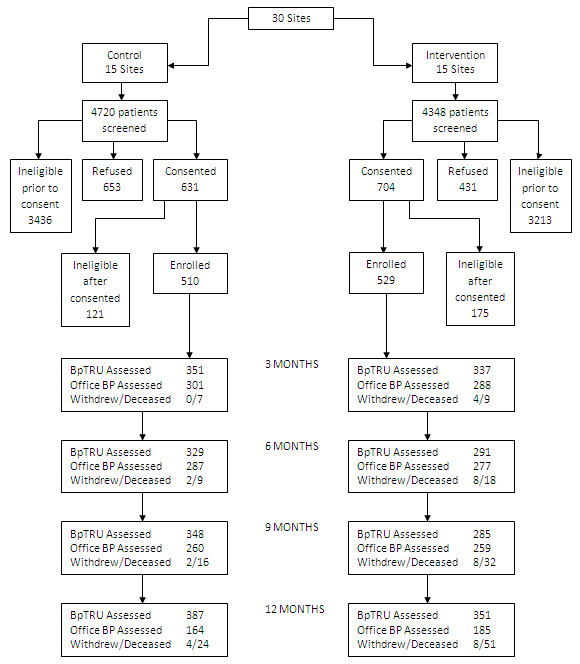
Participants included 1,039 hypertensive African Americans receiving care in 30 CHCs in the New York Metropolitan area. Baseline data on participant demographic, clinical (e.g., BP, anti-hypertensive medications), psychosocial (e.g., depression, medication adherence, self-efficacy), and behavioral (e.g., exercise, diet) characteristics were gathered through direct observation, chart review, and interview.
The sample was primarily female (71.6%), middle-aged (mean age = 56.9 ± 12.1 years), high school educated (62.4%), low-income (72.4% reporting less than $20,000/year income), and received Medicaid (35.9%) or Medicare (12.6%). Mean systolic and diastolic BP were 150.7 ± 16.7 mm Hg and 91.0 ± 10.6 mm Hg, respectively. Participants were prescribed an average of 2.5 ± 1.9 antihypertensive medications; 54.8% were on a diuretic; 33.8% were on a beta blocker; 41.9% were on calcium channel blockers; 64.8% were on angiotensin converting enzyme (ACE) inhibitors/angiotensin receptor blockers (ARBs). One-quarter (25.6%) of the sample had resistant hypertension; one-half (55.7%) reported medication non-adherence. Most (79.7%) reported one or more co-morbid medical conditions. The majority of the patients had a Charlson Co-morbidity score ≥ 2. Diabetes mellitus was common (35.8%), and moderate/severe depression was present in 16% of participants. Participants were sedentary (835.3 ± 1,644.2 Kcal burned per week), obese (59.7%), and had poor global physical health, poor eating habits, high health literacy, and good overall mental health.
A majority of patients in the CAATCH trial exhibited adverse lifestyle behaviors, and had significant medical and psychosocial barriers to adequate BP control. Trial outcomes will shed light on the effectiveness of evidence-based interventions for BP control when implemented in real-world medical settings that serve high numbers of low-income hypertensive African-Americans with multiple co-morbidity and significant barriers to behavior change.
在低收入、患有多种合并症的高血压非裔美国人中,联合医生和患者层面的干预措施对血压(BP)控制的有效性在社区初级保健实践中仍在很大程度上未得到检验。描述了参加咨询非裔美国人控制高血压(CAATCH)试验的参与者的人口统计学、临床、心理社会和行为特征。CAATCH 评估了一种多层次、多成分、基于证据的干预措施与常规护理(UC)相比在改善接受社区卫生中心(CHC)初级保健的控制不佳的高血压非裔美国人的 BP 控制方面的有效性。
参与者包括来自纽约大都市区 30 个 CHC 的 1,039 名高血压非裔美国人。通过直接观察、图表审查和访谈收集了参与者人口统计学(例如,BP、抗高血压药物)、心理社会(例如,抑郁、药物依从性、自我效能)和行为(例如,运动、饮食)特征的基线数据。
该样本主要为女性(71.6%)、中年(平均年龄=56.9±12.1 岁)、高中学历(62.4%)、低收入(72.4%报告年收入低于 20,000 美元)和接受医疗补助(35.9%)或医疗保险(12.6%)。平均收缩压和舒张压分别为 150.7±16.7 mmHg 和 91.0±10.6 mmHg。参与者平均开了 2.5±1.9 种降压药;54.8%服用利尿剂;33.8%服用β受体阻滞剂;41.9%服用钙通道阻滞剂;64.8%服用血管紧张素转换酶(ACE)抑制剂/血管紧张素受体阻滞剂(ARB)。四分之一(25.6%)的样本患有难治性高血压;一半(55.7%)报告药物不依从。大多数(79.7%)报告有一个或多个合并症。大多数患者的 Charlson 合并症评分≥2。糖尿病很常见(35.8%),16%的参与者存在中度/重度抑郁。患者久坐不动(每周消耗 835.3±1,644.2 卡路里)、肥胖(59.7%),且整体身体健康状况不佳、饮食习惯不良、健康素养高、整体心理健康状况良好。
CAATCH 试验中的大多数患者表现出不良的生活方式行为,并且在适当控制血压方面存在重大的医疗和心理社会障碍。试验结果将阐明在为服务大量患有多种合并症和行为改变重大障碍的低收入高血压非裔美国人的现实世界医疗环境中实施基于证据的干预措施对血压控制的有效性。