Dolor Rowena J, Yancy William S, Owen William F, Matchar David B, Samsa Gregory P, Pollak Kathryn I, Lin Pao-Hwa, Ard Jamy D, Prempeh Maxwell, McGuire Heather L, Batch Bryan C, Fan William, Svetkey Laura P
Department of Medicine, Duke University Medical Center, Durham, NC, USA.
Trials. 2009 Feb 26;10:13. doi: 10.1186/1745-6215-10-13.
Hypertension affects 29% of the adult U.S. population and is a leading cause of heart disease, stroke, and kidney failure. Despite numerous effective treatments, only 53% of people with hypertension are at goal blood pressure. The chronic care model suggests that blood pressure control can be achieved by improving how patients and physicians address patient self-care.
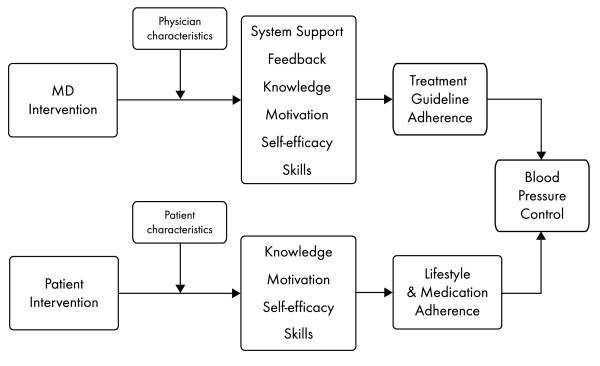
This paper describes the protocol of a nested 2 x 2 randomized controlled trial to test the separate and combined effects on systolic blood pressure of a behavioral intervention for patients and a quality improvement-type intervention for physicians. Primary care practices were randomly assigned to the physician intervention or to the physician control condition. Physician randomization occurred at the clinic level. The physician intervention included training and performance monitoring. The training comprised 2 internet-based modules detailing both the JNC-7 hypertension guidelines and lifestyle modifications for hypertension. Performance data were collected for 18 months, and feedback was provided to physicians every 3 months. Patient participants in both intervention and control clinics were individually randomized to the patient intervention or to usual care. The patient intervention consisted of a 6-month behavioral intervention conducted by trained interventionists in 20 group sessions, followed by 12 monthly phone contacts by community health advisors. Follow-up measurements were performed at 6 and 18 months. The primary outcome was the mean change in systolic blood pressure at 6 months. Secondary outcomes were diastolic blood pressure and the proportion of patients with adequate blood pressure control at 6 and 18 months.
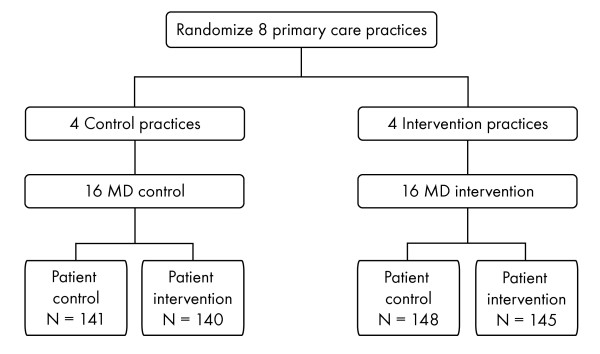
Overall, 8 practices (4 per treatment group), 32 physicians (4 per practice; 16 per treatment group), and 574 patients (289 control and 285 intervention) were enrolled. Baseline characteristics of patients and providers and the challenges faced during study implementation are presented. The HIP interventions may improve blood pressure control and lower cardiovascular disease risk in a primary care practice setting by addressing key components of the chronic care model. The study design allows an assessment of the effectiveness and cost of physician and patient interventions separately, so that health care organizations can make informed decisions about implementation of 1 or both interventions in the context of local resources.
ClinicalTrials.gov identifier NCT00201136.
高血压影响着29%的美国成年人口,是心脏病、中风和肾衰竭的主要病因。尽管有许多有效的治疗方法,但只有53%的高血压患者血压控制达标。慢性病护理模式表明,通过改善患者和医生处理患者自我护理的方式,可以实现血压控制。
本文描述了一项嵌套式2×2随机对照试验的方案,以测试针对患者的行为干预和针对医生的质量改进型干预对收缩压的单独及联合影响。初级保健机构被随机分配到医生干预组或医生对照组。医生随机分组在诊所层面进行。医生干预包括培训和绩效监测。培训包括2个基于互联网的模块,详细介绍了JNC-7高血压指南和高血压的生活方式改变。收集了18个月的绩效数据,并每3个月向医生提供一次反馈。干预诊所和对照诊所的患者参与者被分别随机分配到患者干预组或常规护理组。患者干预包括由经过培训的干预人员在20次小组会议上进行为期6个月的行为干预,随后由社区健康顾问每月进行12次电话随访。在6个月和18个月时进行随访测量。主要结局是6个月时收缩压的平均变化。次要结局是舒张压以及6个月和18个月时血压控制达标的患者比例。
总体而言,共纳入了8个机构(每个治疗组4个)、32名医生(每个机构4名;每个治疗组16名)和574名患者(289名对照和285名干预组)。呈现了患者和提供者的基线特征以及研究实施过程中面临的挑战。通过解决慢性病护理模式的关键组成部分,HIP干预可能会改善初级保健机构环境中的血压控制并降低心血管疾病风险。该研究设计允许分别评估医生和患者干预的有效性和成本,以便医疗保健组织能够根据当地资源就是否实施一种或两种干预做出明智的决策。
ClinicalTrials.gov标识符NCT00201136。