Fundacion Huesped, Buenos Aires, Argentina.
PLoS One. 2011;6(8):e23726. doi: 10.1371/journal.pone.0023726. Epub 2011 Aug 19.
To compare the efficacy and safety of an individualized treatment-simplification strategy consisting of switching from a highly-active anti-retroviral treatment (HAART) with a ritonavir-boosted protease inhibitor (PI/r) and 2 nucleoside reverse-transcriptase inhibitors (NRTIs) to lopinavir/ritonavir (LPV/r) monotherapy, with intensification by 2 NRTIs if necessary, to that of continuing their HAART.
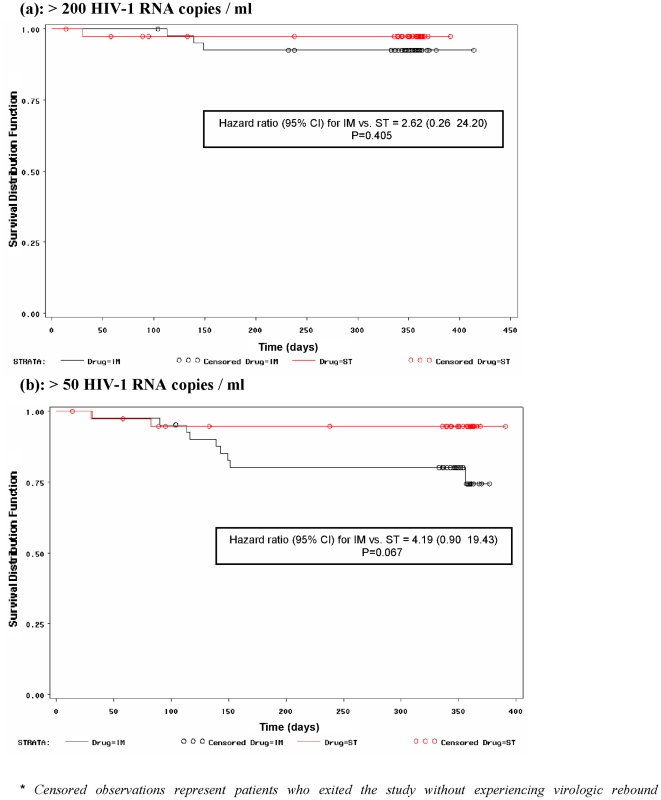
This is a one-year, randomized, open-label, multi-center study in virologically-suppressed HIV-1-infected adults on their first PI/r-containing treatment, randomized to either LPV/r-monotherapy or continue their current treatment. Treatment efficacy was determined by plasma HIV-1 RNA viral load (VL), time-to-virologic rebound, patient-reported outcomes (PROs) and CD4+T-cell-count changes. Safety was assessed with the incidence of treatment-emergent adverse events (AE).
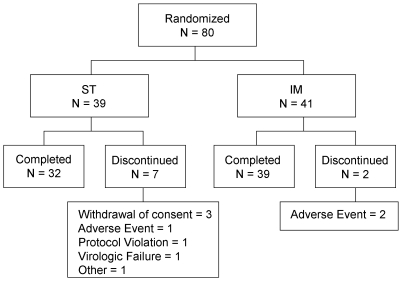
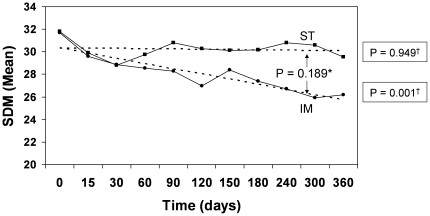
Forty-one patients were randomized to LPV/r and 39 to continue their HAART. No statistically-significant differences between the two study groups in demographics and baseline characteristics were observed. At day-360, 71(39:LPV/r;32:HAART) patients completed treatment, while 9(2:LPV/r;7:HAART) discontinued. In a Last Observation Carried Forward Intent-to-Treat analysis, 40(98%) patients on LPV/r and 37(95%) on HAART had VL<200 copies/mL (P = 0.61). Time-to-virologic rebound, changes in PROs, CD4+ T-cell-count and VL from baseline, also exhibited no statistically-significant between-group differences. Most frequent AEs were diarrhea (19%), headache (18%) and influenza (16%). Four (10%) patients on LPV/r were intensified with 2 NRTIs, all regaining virologic control. Eight serious AEs were reported by 5(2:LPV/r;3:HAART) patients.
At day-360, virologic efficacy and safety of LPV/r appears comparable to that of a PI+2NRTIs HAART. These results suggest that our individualized, simplified maintenance strategy with LPV/r-monotherapy and protocol-mandated NRTI re-introduction upon viral rebound, in virologically-suppressed patients merits further prospective long-term evaluation.
ClinicalTrials.gov NCT00159224.
比较个体化治疗简化策略的疗效和安全性,该策略包括从含利托那韦的蛋白酶抑制剂(PI/r)和 2 种核苷逆转录酶抑制剂(NRTIs)的高效抗逆转录病毒治疗(HAART)转换为洛匹那韦/利托那韦(LPV/r)单药治疗,如果必要,通过 2 种 NRTIs 强化治疗,与继续其 HAART 进行比较。
这是一项为期 1 年、随机、开放标签、多中心研究,纳入了首次接受含 PI/r 治疗的病毒学抑制的 HIV-1 感染成人,随机分为 LPV/r 单药治疗组或继续其当前治疗组。通过血浆 HIV-1 RNA 病毒载量(VL)、病毒学反弹时间、患者报告结局(PRO)和 CD4+T 细胞计数变化来评估治疗效果。通过治疗中出现的不良事件(AE)的发生率来评估安全性。
41 例患者被随机分配至 LPV/r 组,39 例患者被随机分配至继续其 HAART。两组患者在人口统计学和基线特征方面无统计学显著差异。在第 360 天,71 例(39:LPV/r;32:HAART)患者完成治疗,9 例(2:LPV/r;7:HAART)患者停药。在意向治疗的最后观察结转分析中,40 例(98%)LPV/r 组和 37 例(95%)HAART 组的 VL<200 拷贝/mL(P=0.61)。病毒学反弹时间、PROs、CD4+T 细胞计数和 VL 自基线的变化也没有组间统计学显著差异。最常见的 AE 是腹泻(19%)、头痛(18%)和流感(16%)。4 例(10%)LPV/r 组患者加用 2 种 NRTI 强化治疗,均恢复病毒学控制。5 例(2:LPV/r;3:HAART)患者报告了 8 例严重 AE。
在第 360 天,LPV/r 的病毒学疗效和安全性似乎与含 PI+2NRTIs 的 HAART 相当。这些结果表明,我们的个体化、简化维持策略,在病毒学抑制的患者中,使用 LPV/r 单药治疗,并在病毒反弹时根据方案规定重新引入 NRTI,值得进一步进行前瞻性长期评估。
ClinicalTrials.gov NCT00159224。