Endo Yuichiro, Minato Haruka, Taki Reiko, Kato Mayumi, Kore-Eda Satoshi, Miyachi Yoshiki, Tanioka Miki
Department of Dermatology, Graduate School of Medicine, Kyoto University, Kyoto, Japan.
Case Rep Dermatol. 2011 Jan;3(1):22-7. doi: 10.1159/000324422. Epub 2011 Feb 5.
To report a case of a patient with myeloperoxidase-antineutrophil cytoplasmic antibody (ANCA)-negative microscopic polyangiitis (MPA) and IgA nephropathy associated with severe pulmonary haemorrhage.
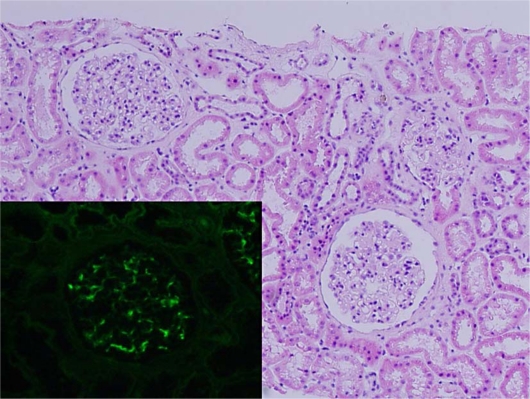
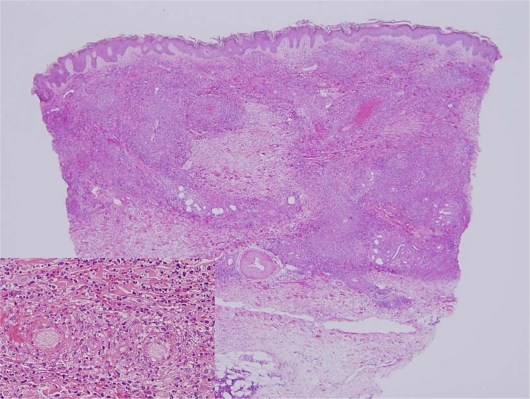
A 59-year-old man presented with ANCA-negative systemic vasculitis accompanied by purpura, nephritis and pulmonary haemorrhage. A skin biopsy specimen revealed pandermal leucocytoclastic vasculitis without IgA deposition and a kidney biopsy showed mesangial nephritis with IgA deposition. Considering these findings, the patient was diagnosed as having MPA with IgA nephropathy.
In most cases, MPA presents with rapidly progressive necrotizing glomerulonephritis and sometimes lung haemorrhage, while IgA nephropathy is less common among MPA cases. As recent research suggested that in MPA immunoglobulin deposition in the kidney may be an exacerbating factor for renal dysfunction and poor prognosis, close observation is required in these cases.
报告1例髓过氧化物酶抗中性粒细胞胞浆抗体(ANCA)阴性的显微镜下多血管炎(MPA)合并IgA肾病且伴有严重肺出血的患者。
一名59岁男性,表现为ANCA阴性的系统性血管炎,伴有紫癜、肾炎和肺出血。皮肤活检标本显示全层白细胞破碎性血管炎,无IgA沉积,肾脏活检显示系膜性肾炎伴IgA沉积。综合这些发现,该患者被诊断为MPA合并IgA肾病。
在大多数情况下,MPA表现为快速进展性坏死性肾小球肾炎,有时伴有肺出血,而IgA肾病在MPA病例中较少见。由于最近的研究表明,在MPA中肾脏免疫球蛋白沉积可能是肾功能障碍和预后不良的一个加重因素,因此对这些病例需要密切观察。