Department of Medicine, King Faisal Specialist Hospital and Research Center, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia.
Ann Thorac Med. 2011 Oct;6(4):207-11. doi: 10.4103/1817-1737.84774.
There is an uncertainty about what constitutes an optimal level of blood glucose (BG) in critically ill patients. The objective of this study is to identify the optimal BG target for glycemic control in critically ill patients that is associated with survival benefit with the least hypoglycemia risk.
This is a nested cohort study within a randomized control trial conducted in a tertiary care center in King Abdulaziz Medical City, Riyadh, Kingdom of Saudi Arabia.
The study was carried out in a single center to assess the effect of intensive insulin therapy [IIT; target BG 4.4-6.1 mmol/L (80-110 mg/dL)] versus conventional insulin therapy [CIT; target BG 10-11.1 mmol/L (180-200 mg/dL)] in a medical/surgical ICU. All patients were divided into six groups based on the mean daily BG levels. A logistic regression model was used to determine the association of BG and ICU mortality. We compared different outcomes below and above different BG thresholds of 0.1 mmol/L (2 mg/dL) increments using multivariate analyses.
Data are presented as mean ± SD or median with interquartile ranges, unless otherwise indicated. Differences between the six groups were assessed using the χ(2) test. A P-value equal or less than 0.05 was considered to indicate statistical significance. The results were expressed as adjusted odds ratio (aOR) and 95% confidence intervals (CI). Statistical analyses were carried out using the Statistical Analysis Software (SAS, release 8, SAS Institute Inc., Cary, NC, USA).
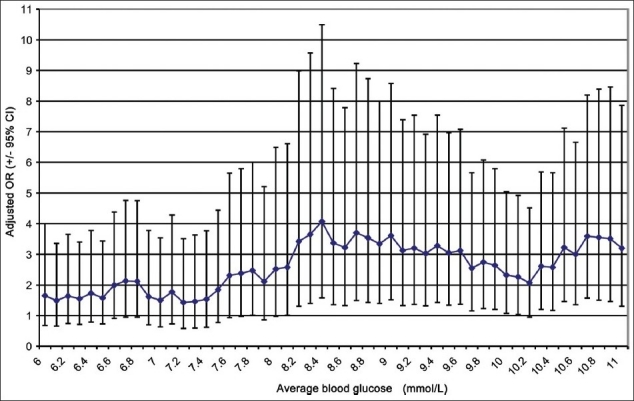
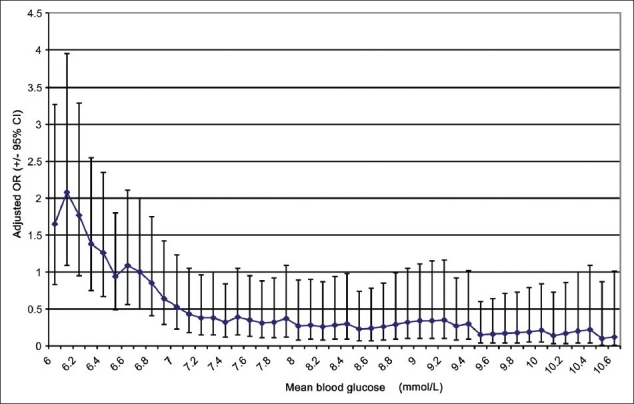
Among six groups, the ICU mortality was least in patients with BG <8.7 mmol/L (<157 mg/dL) compared with patients with BG ≥8.7 mmol/L (≥157 mg/dL) [11.5% vs. 21.5%, P = 0.002]. When analyzed using 0.1 mmol increments in average BG, we found that mortality remained unchanged by increasing thresholds of BG up to 8.0 mmol/L (144 mg/dL) and started to rise with thresholds of BG of 8.1 mmol/L (146 mg/dL) and above. The risk of hypoglycemia was the highest with a BG threshold of 6.1 mmol/L (110 mg/dL) and gradually decreased with increasing BG levels to plateau with a BG level of 7.2 mmol/L (130 mg/dL) and higher.
Our study suggests that a BG level of 8.1 mmol/L (146 mg/dL) and below represents an optimal level in critically ill patients.
目前对于危重症患者的血糖(BG)最佳水平仍存在不确定性。本研究旨在确定与低血糖风险最小化相关的、能使危重症患者获得生存获益的最佳血糖控制目标。
这是在沙特阿拉伯利雅得阿卜杜勒阿齐兹国王医疗城的一家三级护理中心进行的一项随机对照试验中的嵌套队列研究。
该研究在一家单中心进行,以评估强化胰岛素治疗(目标 BG 4.4-6.1 mmol/L [80-110mg/dL])与常规胰岛素治疗(目标 BG 10-11.1mmol/L [180-200mg/dL])在重症监护病房(ICU)中对危重症患者的影响。所有患者均根据平均每日 BG 水平分为六组。采用逻辑回归模型确定 BG 与 ICU 死亡率之间的关联。我们使用多变量分析比较了不同 BG 阈值(每增加 0.1mmol/L [2mg/dL])以下和以上的不同结果。
数据表示为平均值±标准差或中位数和四分位距,除非另有说明。使用 χ(2)检验比较六组之间的差异。P 值等于或小于 0.05 被认为具有统计学意义。结果表示为调整后的优势比(aOR)和 95%置信区间(CI)。使用统计分析软件(SAS,版本 8,SAS Institute Inc.,Cary,NC,USA)进行统计分析。
在六组患者中,BG<8.7mmol/L(<157mg/dL)的患者 ICU 死亡率最低,而 BG≥8.7mmol/L(≥157mg/dL)的患者 ICU 死亡率最高[11.5%比 21.5%,P=0.002]。当以平均 BG 增加 0.1mmol 进行分析时,我们发现,BG 阈值增加至 8.0mmol/L(144mg/dL)时死亡率保持不变,而 BG 阈值增加至 8.1mmol/L(146mg/dL)及以上时死亡率开始上升。BG 阈值为 6.1mmol/L(110mg/dL)时发生低血糖的风险最高,随着 BG 水平的升高逐渐降低,BG 水平为 7.2mmol/L(130mg/dL)及更高时风险趋于平稳。
我们的研究表明,BG 水平为 8.1mmol/L(146mg/dL)及以下是危重症患者的最佳水平。