Department of Obstetrics and Gynecology, the Catholic University, Seoul, Korea.
World J Surg Oncol. 2011 Oct 11;9:123. doi: 10.1186/1477-7819-9-123.
Malignant ovarian germ cell tumors are rare, and knowledge of their prognostic factors is limited, with little available randomized data. This study was conducted to evaluate the clinicopathologic characteristics of malignant ovarian germ cell tumors and to determine the association of their prognostic factors to primary treatment failure.
The medical records of 57 patients with stages I to IV malignant ovarian germ cell tumor were retrospectively reviewed, and their clinicopathologic and treatment-related data were collected and analyzed.
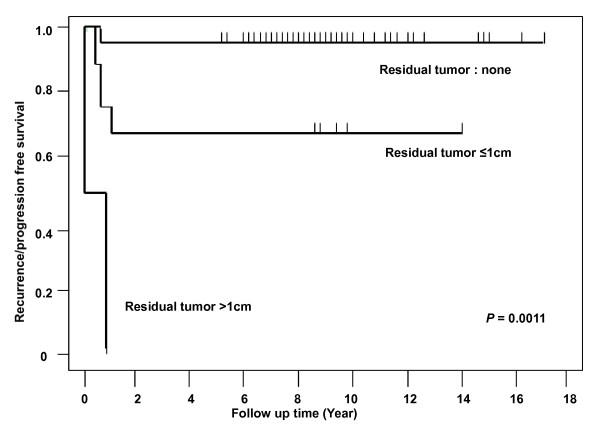
The median age at the diagnosis was 23.3 years (range: 8-65 years), and the median follow-up period was 108 months (range: 48-205 months). The histological types of the tumors were immature teratoma (n = 24), dysgerminoma (n = 20), endodermal sinus tumor (n = 8), mixed germ cell tumor (n = 4), and choriocarcinoma (n = 1). 66.7% of the patients had stage I disease; 5.2%, stage II; 26.3%, stage III; and 1.8%, stage IV. After the initial surgery, 49 patients (86%) received cisplatin-based chemotherapy. The five-year survival rate was 96.5%. There were six primary treatment failures, with two of the patients dying of the disease, and the median time to the recurrence was 8 months. The histological diagnosis (P < 0.0001), tumor stage (P = 0.0052), elevation of beta-hCG (P = 0.0134), operation methods (P = 0.0006), and residual tumor after the salvage surgery (P < 0.0001) were significantly associated with the risk of primary treatment failure in the univariate analysis. In the multivariate analysis, the residual tumor after the salvage surgery was the only significant variable associated with primary treatment failure (P = 0.0011, Hazard ratio = 29.046, 95% Confidence interval 3.832-220.181).
Most malignant ovarian germ cell tumors have excellent prognoses with primary treatment, and good reproductive outcomes can be expected. Because primary treatment failure is associated with the residual disease after the salvage surgery, knowledge of the presence or absence of this risk factor may be helpful in risk stratification and individualization of adjuvant therapy in malignant ovarian germ cell tumors. Further large-scale prospective studies to confirm these results should be performed.
卵巢恶性生殖细胞肿瘤较为罕见,其预后因素的相关知识有限,且随机数据较少。本研究旨在评估卵巢恶性生殖细胞肿瘤的临床病理特征,并确定其预后因素与原发治疗失败的相关性。
回顾性分析 57 例Ⅰ至Ⅳ期卵巢恶性生殖细胞肿瘤患者的病历资料,收集并分析其临床病理和治疗相关数据。
中位发病年龄为 23.3 岁(范围:8-65 岁),中位随访时间为 108 个月(范围:48-205 个月)。肿瘤的组织学类型为:未成熟畸胎瘤(n=24)、无性细胞瘤(n=20)、内胚窦瘤(n=8)、混合性生殖细胞肿瘤(n=4)和绒癌(n=1)。66.7%的患者为Ⅰ期疾病,5.2%为Ⅱ期,26.3%为Ⅲ期,1.8%为Ⅳ期。初始手术后,49 例(86%)患者接受了顺铂为基础的化疗。5 年生存率为 96.5%。有 6 例原发治疗失败,其中 2 例死于疾病,复发的中位时间为 8 个月。组织学诊断(P<0.0001)、肿瘤分期(P=0.0052)、β-hCG 升高(P=0.0134)、手术方式(P=0.0006)和挽救性手术后的残留肿瘤(P<0.0001)在单因素分析中与原发治疗失败的风险显著相关。多因素分析显示,挽救性手术后的残留肿瘤是与原发治疗失败相关的唯一显著变量(P=0.0011,风险比=29.046,95%置信区间 3.832-220.181)。
大多数卵巢恶性生殖细胞肿瘤经原发治疗后预后良好,可获得良好的生殖结局。由于原发治疗失败与挽救性手术后的残留疾病相关,了解是否存在该风险因素可能有助于对卵巢恶性生殖细胞肿瘤进行风险分层和辅助治疗的个体化。应开展进一步的大规模前瞻性研究以验证这些结果。