Baranchuk Adrian, McIntyre William, Harper William, Morillo Carlos A
Queen's University, Arrhythmia Service, Kingston, ON, Canada.
Indian Pacing Electrophysiol J. 2011 Sep;11(5):134-44. Epub 2011 Oct 2.
The goals of this study were to apply the 2001 ACEP recommendations for admission to hospital after a syncopal event and to validate the OESIL risk stratification score, in patients with syncope admitted to a general internal medicine ward.
A retrospective study applied the 2001 ACEP recommendations and OESIL score to all the patients admitted from the emergency department to a general internal medicine ward with a diagnosis of syncope during a 12-month period. The patients were classified as meeting criteria for 2001 ACEP class B or C recommendations and OESIL score 0-1 (low-risk for a major cardiac event) or 2-4 (high-risk for a major cardiac event). The sensitivity and specificity of each group for predicting high-risk patients was calculated.
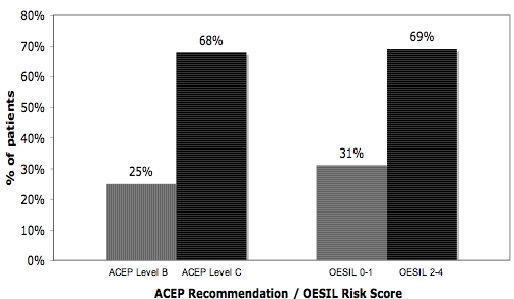
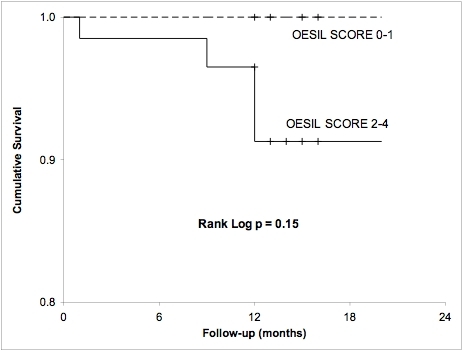
After applying the 2001 ACEP recommendations to our population, 25% (19 patients) were classified as level B, whereas 68% of the patients were classified as Level C. Sensitivity for ACEP level B recommendations was 100% and specificity was 81%. The ACEP level C recommendations also had 100% sensitivity but markedly reduced specificity at 26%. An OESIL score of 0-1 points was calculated for 30.6% of the population, identifying them as low-risk. An OESIL score of 2-4 points was documented in the remaining 69.4% with a mortality risk of 20 % /year.
A significant proportion (30%) of patients presenting with syncope to a tertiary care University Hospital emergency department and admitted to an Internal Medicine ward were retrospectively classified as low-risk and could have potentially been managed as outpatients. Implementing current guidelines and clinical pathways for the management of syncope may improve this approach.
本研究的目标是应用2001年美国急诊医师学会(ACEP)关于晕厥事件后入院的建议,并验证OESIL风险分层评分,研究对象为入住普通内科病房的晕厥患者。
一项回顾性研究将2001年ACEP建议和OESIL评分应用于在12个月期间从急诊科收治到普通内科病房且诊断为晕厥的所有患者。患者被分类为符合2001年ACEP B级或C级建议标准,以及OESIL评分为0 - 1分(重大心脏事件低风险)或2 - 4分(重大心脏事件高风险)。计算每组预测高风险患者的敏感性和特异性。
将2001年ACEP建议应用于我们的研究人群后,25%(19例患者)被分类为B级,而68%的患者被分类为C级。ACEP B级建议的敏感性为100%,特异性为81%。ACEP C级建议的敏感性也为100%,但特异性显著降低,为26%。30.6%的人群OESIL评分为0 - 1分,被确定为低风险。其余69.4%的人群OESIL评分为2 - 4分,年死亡风险为20%。
在一家三级医疗大学医院急诊科就诊并入住内科病房的晕厥患者中,相当比例(30%)的患者经回顾性分类为低风险,可能原本可以作为门诊患者处理。实施当前晕厥管理指南和临床路径可能会改善这种处理方式。