Infections and Immunoepidemiology Branch, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, DHHS, Rockville, MD 20852, USA.
Infect Agent Cancer. 2011 Oct 17;6(1):16. doi: 10.1186/1750-9378-6-16.
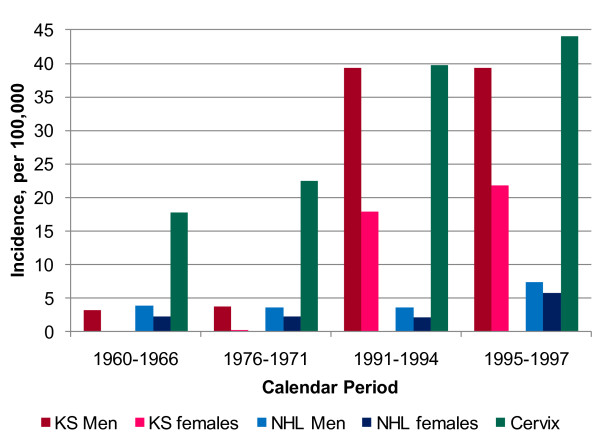
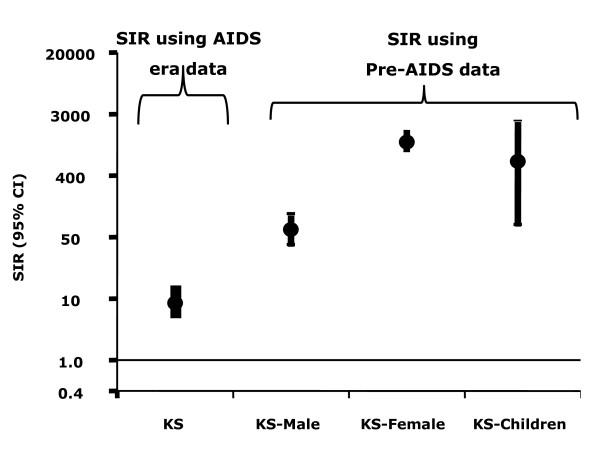
The eruption of Kaposi sarcoma (KS) and aggressive non-Hodgkin lymphoma (NHL) in young homosexual men in 1981 in the West heralded the onset of the human immunodeficiency virus (HIV) infection epidemic, which remains one of the biggest challenges to global public health and science ever. Because KS and NHL were increased >10,000 and 50-600 times, respectively, with HIV, they were designated AIDS defining cancers (ADC). Cervical cancer (CC), increased 5-10 times was also designated as an ADC. A few other cancers are elevated with HIV, including Hodgkin lymphoma (10 times), anal cancer (15-30 times), and lung cancer (4 times) are designated as non-AIDS defining cancers (NADCs). Since 1996 when combination antiretroviral therapy (cART) became widely available in the West, dramatic decreases in HIV mortality have been observed and substantial decrease in the incidence of ADCs. Coincidentally, the burden of NADCs has increased as people with HIV age with chronic HIV infection. The impact of HIV infection on cancer in sub-Saharan Africa, where two thirds of the epidemic is concentrated, remains poorly understood. The few studies conducted indicate that risks for ADCs are also increased, but quantitatively less so than in the West. The risks for many cancers with established viral associations, including liver and nasopharynx, which are found in Africa, do not appear to be increased. These data are limited because of competing mortality, and cancer is under diagnosed, pathological confirmation is rare, and cancer registration not widely practiced. The expansion of access to life-extending cART in sub-Saharan Africa, through programs such as the Global Fund for AIDS, Malaria, and Tuberculosis and the US President's Emergency Program for AIDS Relief (PEPFAR), is leading to dramatic lengthening of life of HIV patients, which will likely influence the spectrum and burden of cancer in patients with HIV. In this paper, we review current literature and explore merits for integrating cancer research in established HIV programs to obtain timely data about the incidence and burden of cancer in HIV-infected persons in Africa.
1981 年,西方年轻同性恋男性中卡波西肉瘤(KS)和侵袭性非霍奇金淋巴瘤(NHL)的爆发预示着人类免疫缺陷病毒(HIV)感染流行的开始,这仍然是全球公共卫生和科学面临的最大挑战之一。由于 KS 和 NHL 分别增加了 >10000 倍和 50-600 倍,因此被指定为艾滋病定义性癌症(ADC)。宫颈癌(CC)增加了 5-10 倍,也被指定为 ADC。还有一些其他癌症与 HIV 一起升高,包括霍奇金淋巴瘤(10 倍)、肛门癌(15-30 倍)和肺癌(4 倍),被指定为非艾滋病定义性癌症(NADC)。自 1996 年联合抗逆转录病毒疗法(cART)在西方广泛应用以来,HIV 死亡率已大幅下降,ADC 发病率也大幅下降。巧合的是,随着 HIV 感染者年龄的增长,慢性 HIV 感染的 NADCs 负担也在增加。在撒哈拉以南非洲,三分之二的艾滋病流行集中在那里,艾滋病毒感染对癌症的影响仍知之甚少。少数进行的研究表明,ADC 的风险也增加了,但在数量上不如西方那么多。在那里发现的与已建立的病毒关联的许多癌症(包括肝脏和鼻咽癌)的风险似乎并未增加。这些数据是有限的,因为存在竞争死亡率,而且癌症的诊断不足,病理证实很少,癌症登记也没有广泛开展。通过全球艾滋病、疟疾和结核病基金以及美国总统艾滋病紧急救援计划(PEPFAR)等方案,在撒哈拉以南非洲扩大获得延长生命的 cART 的机会,导致 HIV 患者的生命大大延长,这可能会影响 HIV 患者的癌症谱和负担。在本文中,我们回顾了当前的文献,并探讨了将癌症研究纳入既定 HIV 计划的优点,以获得关于非洲 HIV 感染者癌症发病率和负担的及时数据。