Section of Cardiovascular Medicine, Department of Internal Medicine, Yale University School of Medicine, 333 Cedar St, New Haven, CT 06520, USA.
JAMA. 2011 Oct 19;306(15):1669-78. doi: 10.1001/jama.2011.1474.
It is not known whether recent declines in ischemic heart disease and its risk factors have been accompanied by declines in heart failure (HF) hospitalization and mortality.
To examine changes in HF hospitalization rate and 1-year mortality rate in the United States, nationally and by state or territory.
DESIGN, SETTING, AND PARTICIPANTS: From acute care hospitals in the United States and Puerto Rico, 55,097,390 fee-for-service Medicare beneficiaries hospitalized between 1998 and 2008 with a principal discharge diagnosis code for HF.
Changes in patient demographics and comorbidities, HF hospitalization rates, and 1-year mortality rates.
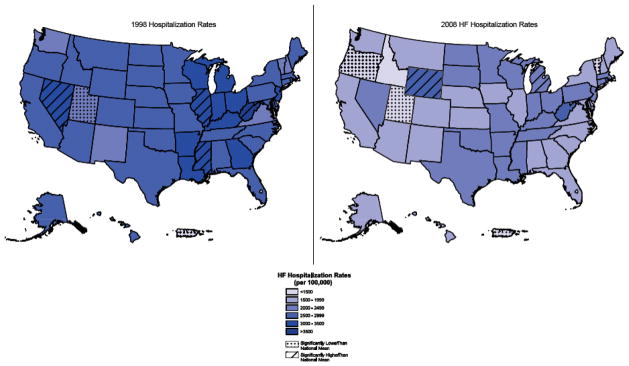
The HF hospitalization rate adjusted for age, sex, and race declined from 2845 per 100,000 person-years in 1998 to 2007 per 100,000 person-years in 2008 (P < .001), a relative decline of 29.5%. Age-adjusted HF hospitalization rates declined over the study period for all race-sex categories. Black men had the lowest rate of decline (4142 to 3201 per 100,000 person-years) among all race-sex categories, which persisted after adjusting for age (incidence rate ratio, 0.81; 95% CI, 0.79-0.84). Heart failure hospitalization rates declined significantly faster than the national mean in 16 states and significantly slower in 3 states. Risk-adjusted 1-year mortality decreased from 31.7% in 1999 to 29.6% in 2008 (P < .001), a relative decline of 6.6%. One-year mortality rates declined significantly in 4 states but increased in 5 states.
The overall HF hospitalization rate declined substantially from 1998 to 2008 but at a lower rate for black men. The overall 1-year mortality rate declined slightly over the past decade but remains high. Changes in HF hospitalization and 1-year mortality rates were uneven across states.
目前尚不清楚缺血性心脏病及其危险因素的近期下降是否伴随着心力衰竭(HF)住院率和死亡率的下降。
在美国全国范围内,以及按州或领地划分,检查 HF 住院率和 1 年死亡率的变化。
设计、地点和参与者:在美国和波多黎各的急性护理医院,1998 年至 2008 年间有 55097390 名 Medicare 自费患者因 HF 的主要出院诊断代码住院。
患者人口统计学和合并症、HF 住院率和 1 年死亡率的变化。
经年龄、性别和种族调整的 HF 住院率从 1998 年至 2007 年的每 10 万人 2845 人/年降至每 10 万人 2008 年的 2007 人/年(P<0.001),相对下降了 29.5%。在整个研究期间,所有种族-性别类别中,年龄调整后的 HF 住院率都有所下降。在所有种族-性别类别中,黑人男性下降率最低(每 10 万人 4142 人至 3201 人/年),在调整年龄后仍保持不变(发病率比,0.81;95%CI,0.79-0.84)。16 个州的 HF 住院率下降速度明显快于全国平均水平,3 个州的下降速度明显慢于全国平均水平。调整风险后的 1 年死亡率从 1999 年的 31.7%降至 2008 年的 29.6%(P<0.001),相对下降了 6.6%。在 4 个州,1 年死亡率显著下降,但在 5 个州,死亡率上升。
从 1998 年到 2008 年,HF 住院率总体大幅下降,但黑人男性的下降速度较慢。过去十年,1 年死亡率略有下降,但仍居高不下。HF 住院和 1 年死亡率的变化在各州之间不均衡。