Sterling Madeline R, Espinosa Cisco G, Spertus Daniel, Shum Michelle, McDonald Margaret V, Ryvicker Miriam B, Barrón Yolanda, Tobin Jonathan N, Kern Lisa M, Safford Monika M, Banerjee Samprit, Goyal Parag, Ringel Joanna Bryan, Rajan Mangala, Arbaje Alicia I, Jones Christine D, Dodson John A, Cené Crystal, Bowles Kathryn H
Department of Medicine, Weill Cornell Medicine, 420 East 70th Street, LH-357, New York, 10065, NY, USA.
Center for Home Care Policy & Research, VNS Health, New York, NY, USA.
BMC Health Serv Res. 2024 Oct 1;24(1):1160. doi: 10.1186/s12913-024-11584-x.
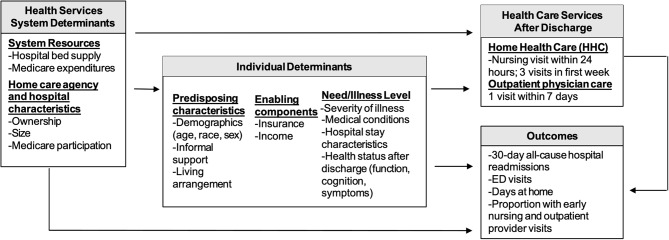
Some of the most promising strategies to reduce hospital readmissions in heart failure (HF) is through the timely receipt of home health care (HHC), delivered by Medicare-certified home health agencies (HHAs), and outpatient medical follow-up after hospital discharge. Yet national data show that only 12% of Medicare beneficiaries receive these evidence-based practices, representing an implementation gap. To advance the science and improve outcomes in HF, we will test the effectiveness and implementation of an intervention called Improving TRansitions ANd OutcomeS for Heart FailurE Patients in Home Health CaRe (I-TRANSFER-HF), comprised of early and intensive HHC nurse visits combined with an early outpatient medical visit post-discharge, among HF patients receiving HHC.
This study will use a Hybrid Type 1, stepped wedge randomized trial design, to test the effectiveness and implementation of I-TRANSFER-HF in partnership with four geographically diverse dyads of hospitals and HHAs ("hospital-HHA" dyads) across the US. Aim 1 will test the effectiveness of I-TRANSFER-HF to reduce 30-day readmissions (primary outcome) and ED visits (secondary outcome), and increase days at home (secondary outcome) among HF patients who receive timely follow-up compared to usual care. Hospital-HHA dyads will be randomized to cross over from a baseline period of no intervention to the intervention in a randomized sequential order. Medicare claims data from each dyad and from comparison dyads selected within the national dataset will be used to ascertain outcomes. Hypotheses will be tested with generalized mixed models. Aim 2 will assess the determinants of I-TRANSFER-HF's implementation using a mixed-methods approach and is guided by the Consolidated Framework for Implementation Research 2.0 (CFIR 2.0). Qualitative interviews will be conducted with key stakeholders across the hospital-HHA dyads to assess acceptability, barriers, and facilitators of implementation; feasibility and process measures will be assessed with Medicare claims data.
As the first pragmatic trial of promoting timely HHC and outpatient follow-up in HF, this study has the potential to dramatically improve care and outcomes for HF patients and produce novel insights for the implementation of HHC nationally.
This trial has been registered on ClinicalTrials.Gov (#NCT06118983). Registered on 10/31/2023, https://clinicaltrials.gov/study/NCT06118983?id=NCT06118983&rank=1 .
减少心力衰竭(HF)患者再入院的一些最具前景的策略是通过及时接受由医疗保险认证的家庭健康机构(HHA)提供的家庭医疗保健(HHC)以及出院后的门诊医疗随访。然而,全国数据显示,只有12%的医疗保险受益人接受这些循证实践,这表明存在实施差距。为了推进心力衰竭领域的科学研究并改善治疗效果,我们将测试一种名为“改善家庭健康护理中心力衰竭患者的过渡与结局”(I-TRANSFER-HF)的干预措施的有效性和实施情况,该措施包括早期和密集的家庭医疗保健护士访视以及出院后的早期门诊医疗访视,针对接受家庭医疗保健的心力衰竭患者。
本研究将采用混合1型阶梯楔形随机试验设计,与美国四个地理位置不同的医院和家庭健康机构二元组(“医院-HHA”二元组)合作,测试I-TRANSFER-HF的有效性和实施情况。目标1将测试I-TRANSFER-HF与常规护理相比,在及时接受随访的心力衰竭患者中减少30天再入院率(主要结局)和急诊就诊次数(次要结局)以及增加在家天数(次要结局)的有效性。医院-HHA二元组将随机按顺序从无干预的基线期过渡到干预期。来自每个二元组以及从国家数据集中选择的对照二元组的医疗保险理赔数据将用于确定结局。假设将使用广义混合模型进行检验。目标2将采用混合方法评估I-TRANSFER-HF实施的决定因素,并以实施研究综合框架2.0(CFIR 2.0)为指导。将对医院-HHA二元组中的关键利益相关者进行定性访谈,以评估实施的可接受性、障碍和促进因素;可行性和过程指标将通过医疗保险理赔数据进行评估。
作为第一项促进心力衰竭患者及时接受家庭医疗保健和门诊随访的务实试验,本研究有可能显著改善心力衰竭患者的护理和结局,并为在全国范围内实施家庭医疗保健产生新的见解。
本试验已在ClinicalTrials.Gov上注册(#NCT06118983)。于2023年10月31日注册,https://clinicaltrials.gov/study/NCT06118983?id=NCT06118983&rank=1 。