Aravind-Zeiss Centre of Excellence in Glaucoma, Aravind Eye Hospital and Postgraduate Institute of Ophthalmology, Tirunelveli, Tamil Nadu - 627 001, India.
Indian J Ophthalmol. 2011 Nov-Dec;59(6):445-53. doi: 10.4103/0301-4738.86311.
To evaluate the microbial etiology and associated risk factors among patients with blebitis following trabeculectomy.
A retrospective analysis of all culture-proven blebitis was performed in patients who underwent trabeculectomy between January 2004 and December 2008. A standardized form was filled out for each patient, documenting sociodemographic features and information pertaining to risk factors. Swabbing of the infected bleb surface was performed for all suspected cases and further subjected to microbiological analysis.
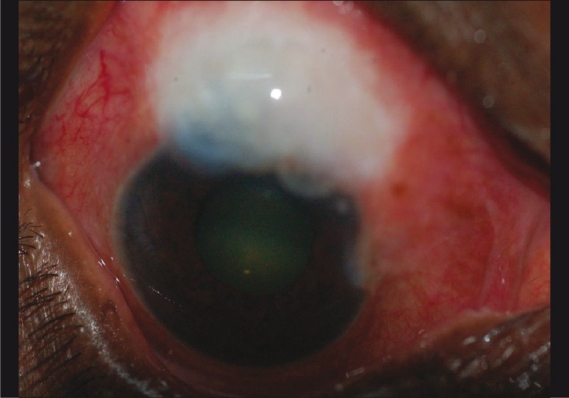
A total of 23 patients with culture-proven blebitis were treated during the study period, with a mean age of 59.2 years (59.2 ± SD: 12.8; range, 30-81 years). Duration of onset was early (≤ 36 months) in six (26%) cases and late (> 36 months) in 17 (74%) cases with a range between 15 and 144 months (mean, 82.91 months; SD: 41.89). All 23 blebs were located superiorly and of which, 21 (91%) were microcystic avascular, 1 (4%) diffuse avascular, and 1 (4%) vascular flattened. The predominant risk factor identified was bleb leak (35%; 8 of 23) followed by thin bleb (22%; 5 of 23) and blepharitis (17%; 4 of 23). Bleb leaks (100%) were recorded only in patients with late onset (≥ 9 years) of infection (P< 0.001), while the incidence of ocular surface disease (100%) occurred early (≤ 3 years) (P< 0.001). Use of topical steroids was associated frequently with cases of thin blebs (80%; 4 of 5) (P< 0.001), while topical antibiotics showed bleb leaks (88%; 7 of 8) (P< 0.001). Coagulase-positive staphylococci were frequently recovered from blebitis with thin blebs (71%; 5 of 7) (P = 0.001), Coagulase-negative staphylococci (CoNS) with bleb leak (100%; 8 of 8) (P< 0.001), Corynebacterium with blepharitis (100%; 3 of 3) (P = 0.001), and Streptococci with releasable sutures (75%; 3 of 4) (P = 0.001).
Bleb leak is the principal risk factor responsible for late-onset blebitis, while early-onset blebitis could be ascribed to ocular surface diseases. Streptococci were mainly responsible for early onset of infection, while the late onset was due to CoNS.
评估小梁切除术后眼内炎的微生物病因及相关危险因素。
对 2004 年 1 月至 2008 年 12 月期间行小梁切除术的患者中所有培养阳性的眼内炎进行回顾性分析。为每位患者填写一份标准表格,记录社会人口统计学特征和与危险因素相关的信息。对所有疑似病例进行感染性滤泡表面拭子取样,并进一步进行微生物分析。
研究期间共治疗了 23 例培养阳性的眼内炎患者,平均年龄 59.2 岁(59.2 ± SD:12.8;范围,30-81 岁)。6 例(26%)为早期(≤36 个月)发病,17 例(74%)为晚期(>36 个月)发病,发病时间为 15-144 个月,平均 82.91 个月(SD:41.89)。所有 23 个滤泡均位于上方,其中 21 个(91%)为微囊无血管型,1 个(4%)为弥漫无血管型,1 个(4%)为血管扁平型。确定的主要危险因素是滤泡渗漏(35%;23 例中的 8 例),其次是滤泡薄(22%;23 例中的 5 例)和睑缘炎(17%;23 例中的 4 例)。仅在感染晚期(≥9 年)(P<0.001)时才记录到滤泡渗漏(100%),而眼表疾病(100%)的发病时间为早期(≤3 年)(P<0.001)。薄滤泡(80%;5 例中的 4 例)(P<0.001)与局部皮质类固醇的使用密切相关,而局部抗生素则与滤泡渗漏(88%;8 例中的 7 例)(P<0.001)有关。凝固酶阳性葡萄球菌经常从薄滤泡(71%;7 例中的 5 例)(P=0.001)中分离出来,凝固酶阴性葡萄球菌(CoNS)与滤泡渗漏(100%;8 例中的 8 例)(P<0.001),睑缘炎(100%;3 例中的 3 例)(P=0.001),和可松解缝线(75%;3 例中的 4 例)(P=0.001)。
滤泡渗漏是导致晚期发病的主要危险因素,而早期发病可归因于眼表疾病。链球菌主要引起早期感染,而晚期发病则与 CoNS 有关。