Intensive Care Unit and Hepatic Hemodynamic Lab, Liver Unit, Hospital Clínic IDIBAPS, University of Barcelona and Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBERehd), 08036 Barcelona, Spain.
Gastroenterol Res Pract. 2011;2011:910986. doi: 10.1155/2011/910986. Epub 2011 Oct 15.
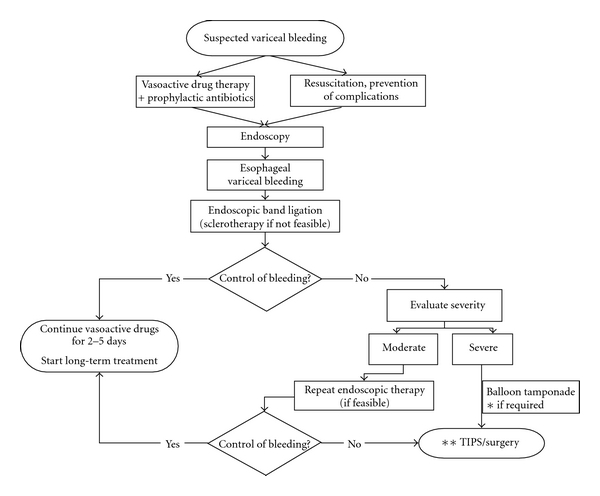
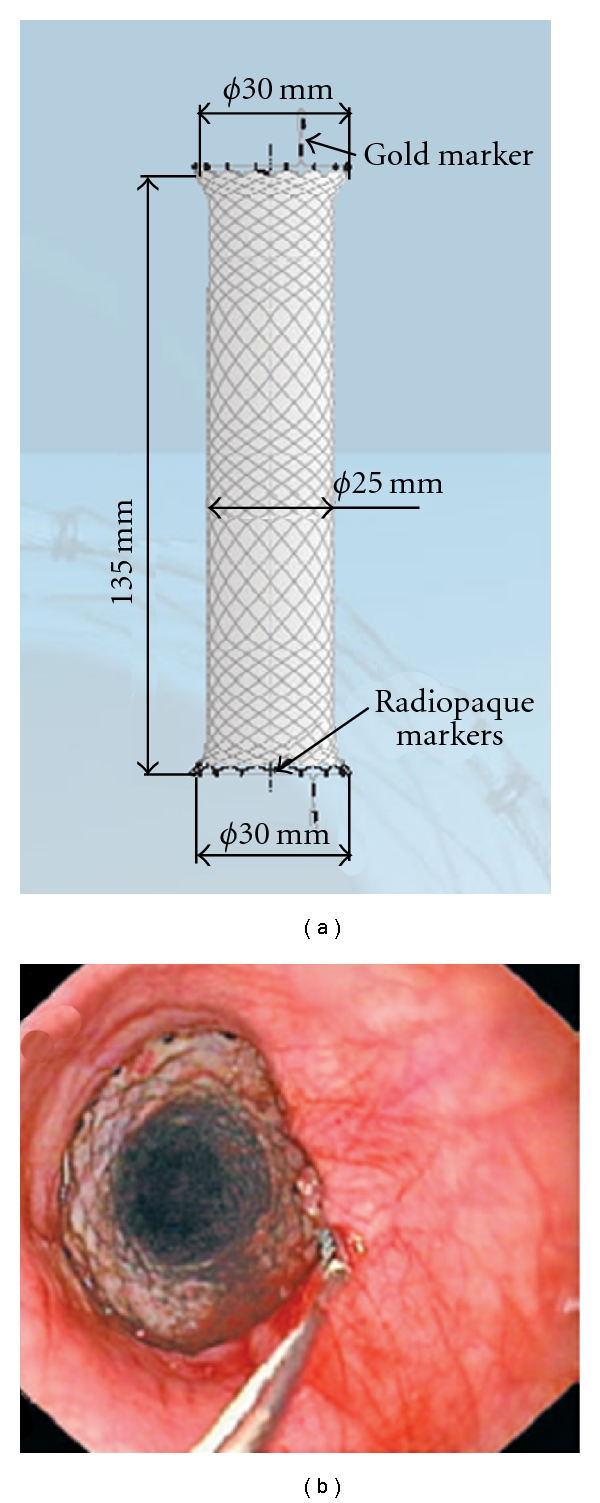
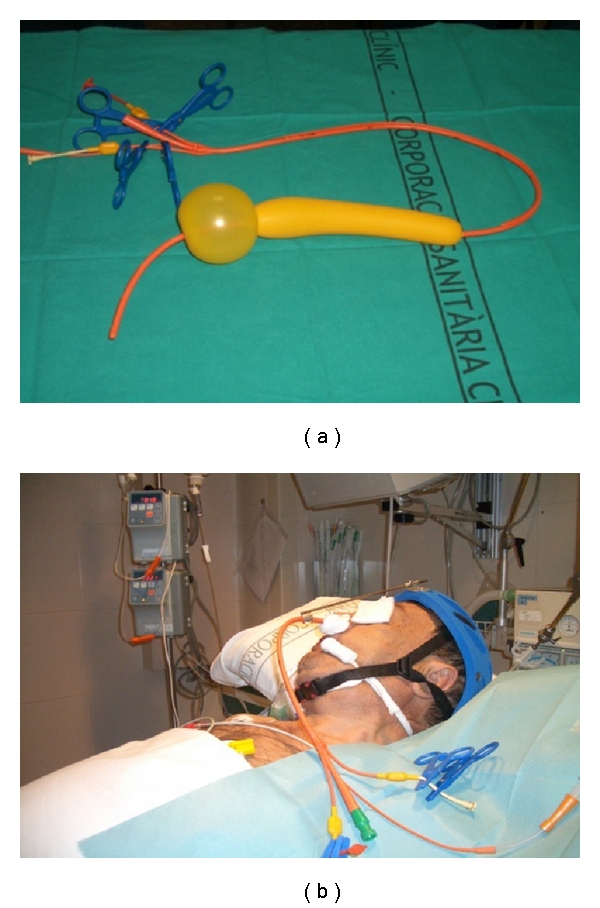
Acute variceal bleeding (AVB) is a life-threatening complication in patients with cirrhosis. Hemostatic therapy of AVB includes early administration of vasoactive drugs that should be combined with endoscopic therapy, preferably banding ligation. However, failure to control bleeding or early rebleed within 5 days still occurs in 15-20% of patients with AVB. In these cases, a second endoscopic therapy may be attempted (mild bleeding in a hemodynamically stable patient) or we can use a balloon tamponade as a bridge to definitive derivative treatment (i.e., a transjugular intrahepatic portosystemic shunt). Esophageal balloon tamponade provides initial control in up to 80% of AVB, but it carries a high risk of major complications, especially in cases of long duration of tamponade (>24 h) and when tubes are inserted by inexperienced staff. Preliminary reports suggest that self-expandable covered esophageal metallic stents effectively control refractory AVB (i.e., ongoing bleeding despite pharmacological and endoscopic therapy or massive bleeding precluding endoscopic therapy) with a low incidence of complications. Thus, covered self-expanding metal stents may represent an alternative to the Sengstaken-Blakemore balloon for the temporary control of bleeding in treatment failures. Further studies are required to determine the role of this new device in AVB.
急性静脉曲张出血 (AVB) 是肝硬化患者的一种危及生命的并发症。AVB 的止血治疗包括早期使用血管活性药物,这些药物应与内镜治疗联合使用,最好是采用套扎治疗。然而,仍有 15-20%的 AVB 患者会出现出血未能得到控制或 5 天内再次出血。在这些情况下,可以尝试再次进行内镜治疗(血流动力学稳定的轻度出血患者),也可以使用气囊填塞作为通向确定性治疗的桥梁(即经颈静脉肝内门体分流术)。食管气囊填塞在高达 80%的 AVB 中可提供初步控制,但它存在严重并发症的高风险,尤其是在填塞时间较长(>24 小时)和由经验不足的人员插入导管的情况下。初步报告表明,自膨式覆膜食管金属支架可有效控制难治性 AVB(即尽管进行了药物和内镜治疗仍持续出血或大量出血而无法进行内镜治疗),并发症发生率较低。因此,覆膜自膨式金属支架可能是治疗失败时替代 Sengstaken-Blakemore 气囊暂时控制出血的一种选择。需要进一步研究来确定这种新设备在 AVB 中的作用。