Desmond Tutu HIV Centre, Institute of Infectious Diseases and Molecular Medicine, University of Cape Town, Cape Town, South Africa.
PLoS One. 2011;6(10):e25098. doi: 10.1371/journal.pone.0025098. Epub 2011 Oct 10.
To describe the burden of tuberculosis (TB) in Cape Town by calculating TB incidence rates stratified by age and HIV-status, assessing the contribution of retreatment disease and estimating the cumulative lifetime TB risk in HIV-negative individuals.
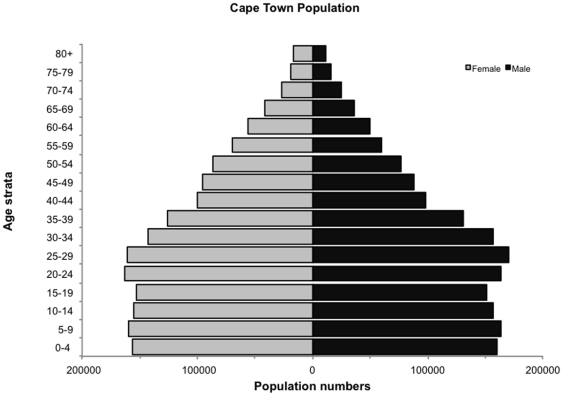
Details of TB cases were abstracted from the 2009 electronic TB register. Population denominators were estimated from census data and actuarial estimates of HIV prevalence, allowing calculation of age-specific and HIV-stratified TB notification rates.
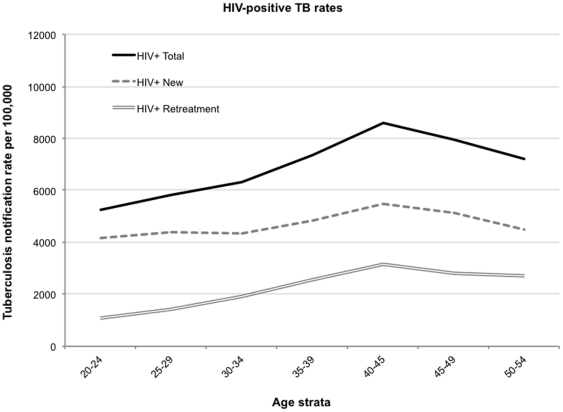
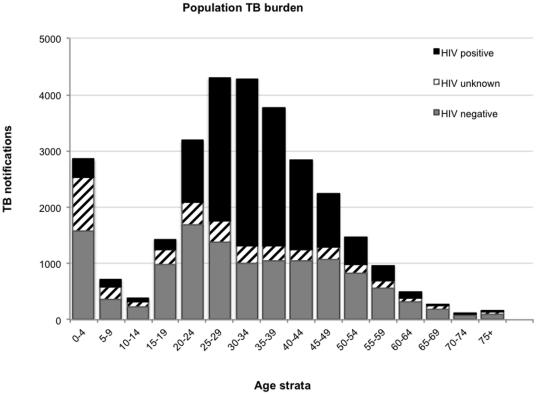
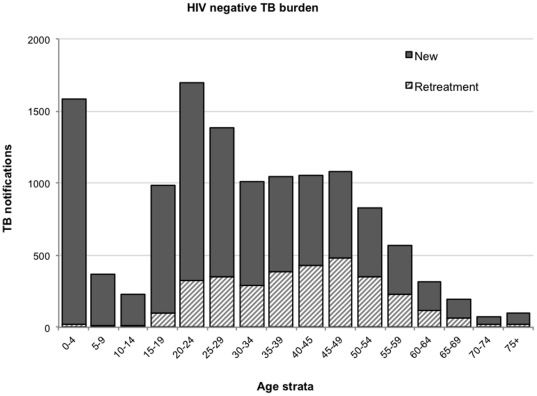
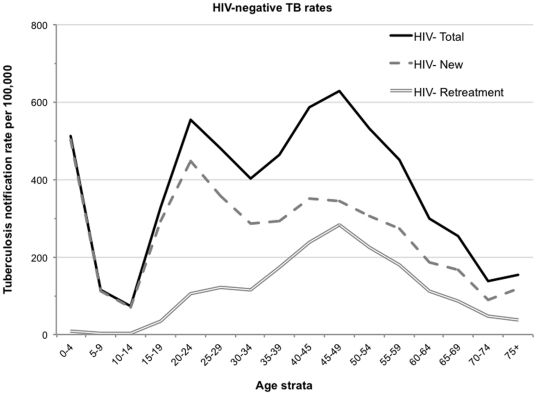
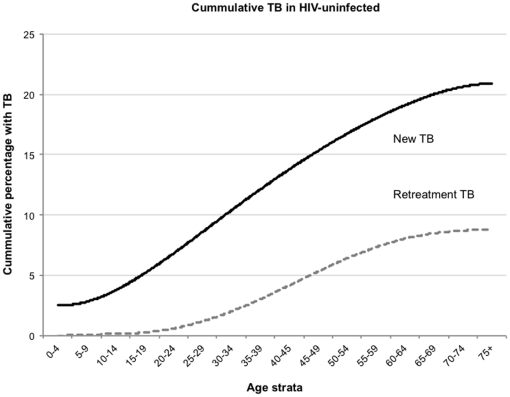
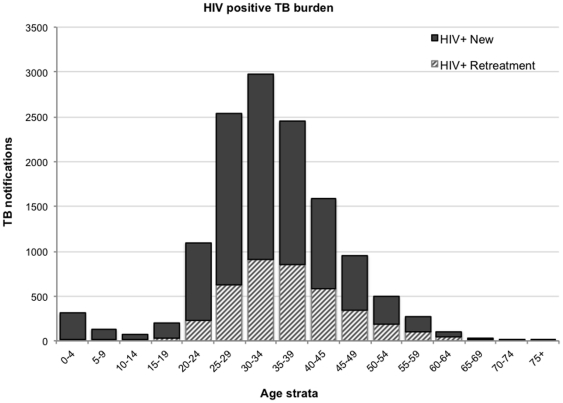
The 2009 mid-year population was 3,443,010 (3,241,508 HIV-negative and 201,502 HIV-positive individuals). There were 29,478 newly notified TB cases of which 56% were laboratory confirmed. HIV status was recorded for 87% of cases and of those with known HIV-status 49% were HIV-negative and 51% were positive. Discrete peaks in the incidence of non-HIV-associated TB occurred at three ages: 511/100,000 at 0-4 years of age, 553/100,000 at 20-24 years and 628/100,000 at 45-49 years with 1.5%, 19% and 45% being due to retreatment TB, respectively. Only 15.5% of recurrent cases had a history of TB treatment failure or default. The cumulative lifetime risks in the HIV-negative population of all new TB episodes and new smear-positive TB episodes were 24% and 12%, respectively; the lifetime risk of retreatment disease was 9%. The HIV-positive notification rate was 6,567/100,000 (HIV-associated TB rate ratio = 17). Although retreatment cases comprised 30% of the HIV-associated TB burden, 88% of these patients had no history of prior treatment failure or default.
The annual burden of TB in this city is huge. TB in the HIV-negative population contributed almost half of the overall disease burden and cumulative lifetime risks were similar to those reported in the pre-chemotherapy era. Retreatment TB contributed significantly to both HIV-associated and non-HIV-associated TB but infrequently followed prior inadequate treatment. This likely reflects ongoing TB transmission to both HIV-negative and positive individuals.
通过计算按年龄和 HIV 状况分层的结核病(TB)发病率,评估复治疾病的贡献,并估计 HIV 阴性个体的累积终身 TB 风险,来描述开普敦的 TB 负担。
从 2009 年电子 TB 登记处提取 TB 病例的详细信息。人口分母由人口普查数据和 HIV 流行率的精算估计数估计,允许计算按年龄和 HIV 分层的 TB 通知率。
2009 年年中人口为 3443010 人(3241508 名 HIV 阴性和 201502 名 HIV 阳性个体)。新报告了 29478 例新的 TB 病例,其中 56%为实验室确诊病例。87%的病例记录了 HIV 状况,在已知 HIV 状况的病例中,49%为 HIV 阴性,51%为阳性。非 HIV 相关 TB 的发病率在三个年龄组出现离散高峰:0-4 岁为 511/100000,20-24 岁为 553/100000,45-49 岁为 628/100000,分别有 1.5%、19%和 45%归因于复治 TB。仅有 15.5%的复发病例有 TB 治疗失败或失约的病史。在 HIV 阴性人群中,所有新发 TB 病例和新发涂片阳性 TB 病例的终身累积风险分别为 24%和 12%;复治疾病的终身风险为 9%。HIV 阳性的通知率为 6567/100000(HIV 相关 TB 率比为 17)。尽管复治病例占 HIV 相关 TB 负担的 30%,但其中 88%的患者没有既往治疗失败或失约的病史。
该市的 TB 年负担巨大。HIV 阴性人群中的 TB 几乎占总疾病负担的一半,累积终身风险与化疗前时代报告的相似。复治 TB 对 HIV 相关和非 HIV 相关 TB 的贡献都很大,但很少是先前治疗不足的结果。这可能反映了 HIV 阴性和阳性个体之间持续的 TB 传播。