Division of Child and Adolescent Psychiatry, Department of Psychiatry, Ohio State University, 1670 Upham Drive, Columbus, OH 43210, USA.
Bipolar Disord. 2011 Aug-Sep;13(5-6):509-21. doi: 10.1111/j.1399-5618.2011.00948.x.
To compare attention-deficit hyperactivity disorder (ADHD), bipolar spectrum disorders (BPSDs), and comorbidity in the Longitudinal Assessment of Manic Symptoms (LAMS) study.
Children ages 6-12 were recruited at first visit to clinics associated with four universities. A BPSD diagnosis required that the patient exhibit episodes. Four hypotheses were tested: (i) children with BPSD + ADHD would have a younger age of mood symptom onset than those with BPSD but no ADHD; (ii) children with BPSD + ADHD would have more severe ADHD and BPSD symptoms than those with only one disorder; (iii) global functioning would be more impaired in children with ADHD + BPSD than in children with either diagnosis alone; and (iv) the ADHD + BPSD group would have more additional diagnoses.
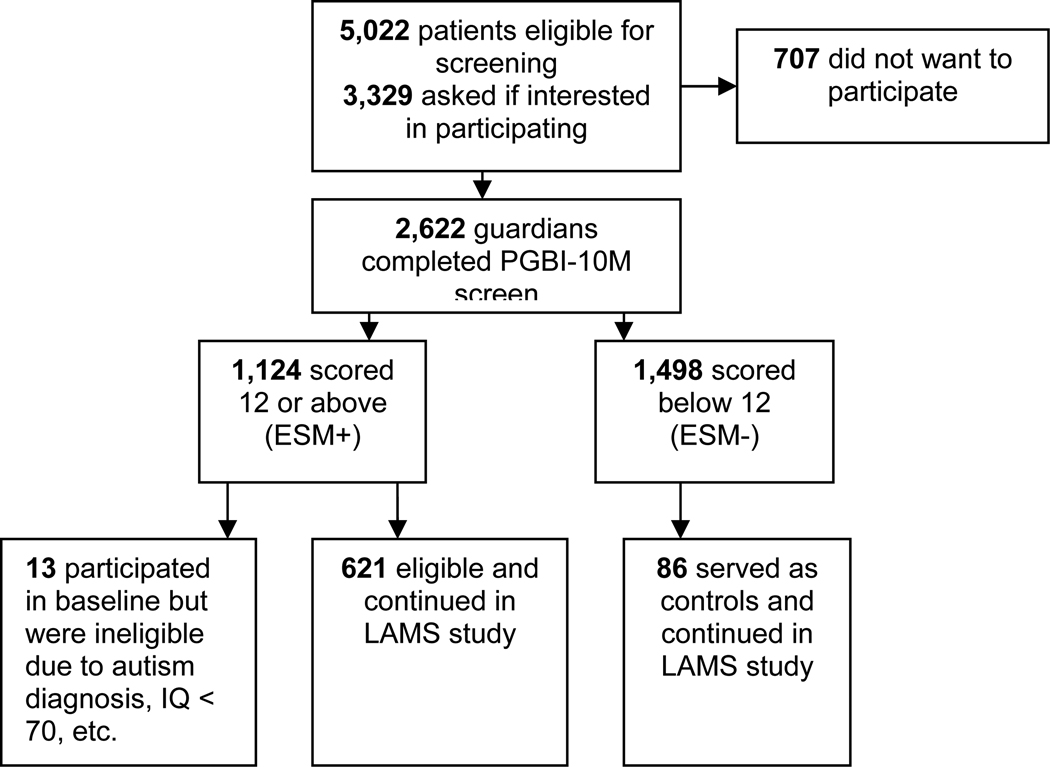
Of 707 children, 421 had ADHD alone, 45 had BPSD alone, 117 had both ADHD and BPSD, and 124 had neither. Comorbidity (16.5%) was slightly less than expected by chance (17.5%). Age of mood symptom onset was not different between the BPSD + ADHD group and the BPSD-alone group. Symptom severity increased and global functioning decreased with comorbidity. Comorbidity with other disorders was highest for the ADHD + BPSD group, but higher for the ADHD-alone than the BPSD-alone group. Children with BPSD were four times as likely to be hospitalized (22%) as children with ADHD alone.
The high rate of BPSD in ADHD reported by some authors may be better explained as a high rate of both disorders in child outpatient settings rather than ADHD being a risk factor for BPSD. Co-occurrence of the two disorders is associated with poorer global functioning, greater symptom severity, and more additional comorbidity than for either single disorder.
比较注意缺陷多动障碍(ADHD)、双相谱系障碍(BPSD)和纵向评估躁狂症状(LAMS)研究中的共病情况。
首次就诊时,从与四所大学相关的诊所招募 6-12 岁的儿童。BPSD 诊断需要患者出现发作。测试了四个假设:(i)有 BPSD+ADHD 的儿童情绪症状发病年龄比只有 BPSD 而没有 ADHD 的儿童年轻;(ii)有 BPSD+ADHD 的儿童的 ADHD 和 BPSD 症状比只有一种疾病的儿童更严重;(iii)在 ADHD+BPSD 儿童中,总体功能障碍比单独一种诊断更严重;(iv)ADHD+BPSD 组的其他诊断更多。
在 707 名儿童中,421 名患有 ADHD 单独,45 名患有 BPSD 单独,117 名患有 ADHD 和 BPSD 两者,124 名患有两者都没有。共病(16.5%)略低于预期的(17.5%)。BPSD+ADHD 组和 BPSD 单独组的情绪症状发病年龄没有差异。随着共病的发生,症状严重程度增加,总体功能下降。与 ADHD+BPSD 组相比,其他疾病的共病发生率最高,而与 BPSD 单独组相比,ADHD 单独组的共病发生率更高。患有 BPSD 的儿童住院的可能性是 ADHD 单独的四倍(22%)。
一些作者报告的 ADHD 中 BPSD 的高发生率可能更好地解释为门诊儿童中这两种疾病的高发生率,而不是 ADHD 是 BPSD 的风险因素。这两种疾病的共病与较差的总体功能、更严重的症状严重程度以及比任何单一疾病更多的其他合并症相关。