Department of Radiotherapy, Saarland University Hospital, Kirrberger Strasse, D-66421 Homburg, Germany.
Radiat Oncol. 2011 Oct 21;6:141. doi: 10.1186/1748-717X-6-141.
Retrospective evaluation of toxicity and results after radiochemotherapy for glioblastoma.
46 patients with histopathologically proven glioblastoma received simultaneous radiochemotherapy (RCT). The mean age at the beginning of therapy was 59 years, the mean Karnofsky performance index 80%. 44 patients had been operated on before radiotherapy, two had not. A total dose of 60 Gy was applied in daily single fractions of 2.0 Gy within six weeks, 75 mg/m2/day Temozolomide were given orally during the whole radiotherapy period.
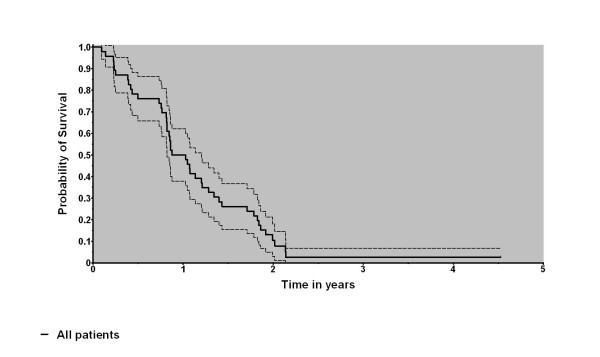
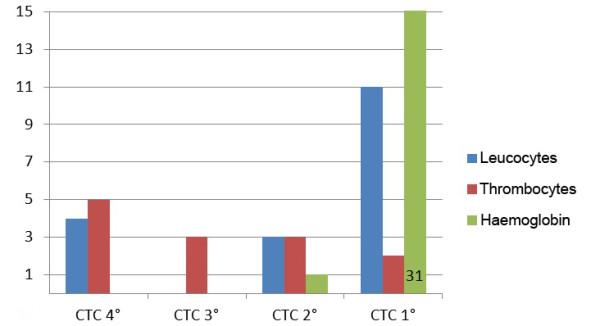
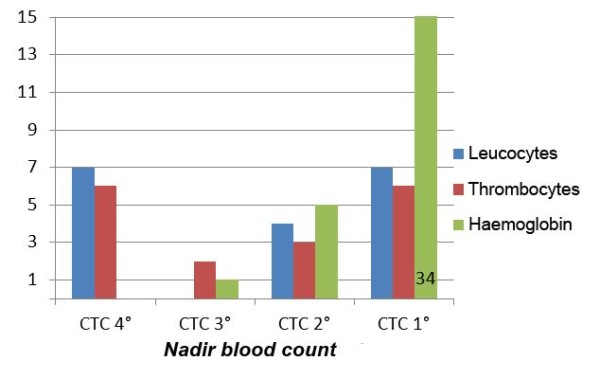
A local progression could be diagnosed in 34/46 patients (70%). The median survival time amounted to 13.6 months resulting in one-year and two-year survival probabilities of 48% and 8%, respectively. Radiotherapy could be applied completely in 89% of the patients. Chemotherapy could be completed according to schedule only in 56.5%, the main reason being blood toxicity (50% of the interruptions). Most of those patients suffered from leucopenia and/or thrombopenia grade III and IV CTC (Common toxicity criteria). Further reasons were an unfavourable general health status or a rise of liver enzymes. The mean duration of thrombopenia and leucopenia amounted to 64 and 20 days. In two patients, blood cell counts remained abnormal until death. In two patients we noticed a rise of liver enzymes. In one of these in the healing phase of hepatitis a rise of ASAT and ALAT CTC grade IV was diagnosed. These values normalized after termination of temozolomide medication. One patient died of pneumonia during therapy.
Our survival data were well within the range taken from the literature. However, we noticed a considerable frequency and intensity of side effects to bone marrow and liver. These lead to the recommendations that regular examinations of blood cell count and liver enzymes should be performed during therapy and temozolomide should not be applied or application should be terminated according to the criteria given by the manufacturer.
回顾性评价胶质母细胞瘤患者放化疗后的毒性和结果。
46 例经组织病理学证实的胶质母细胞瘤患者接受同步放化疗(RCT)。治疗开始时的平均年龄为 59 岁,平均卡诺夫斯基表现指数为 80%。44 例患者在放疗前接受了手术,2 例未接受手术。总剂量为 60 Gy,在 6 周内每日单次剂量 2.0 Gy,在整个放疗期间每天口服 75mg/m2 的替莫唑胺。
46 例患者中有 34 例(70%)可诊断为局部进展。中位生存时间为 13.6 个月,1 年和 2 年生存率分别为 48%和 8%。89%的患者能够完全接受放疗。仅 56.5%的患者能够按照计划完成化疗,主要原因是血液毒性(中断的 50%)。大多数患者患有白细胞减少和/或血小板减少症 III 级和 IV 级 CTC(常见毒性标准)。其他原因包括一般健康状况不佳或肝酶升高。血小板减少和白细胞减少的平均持续时间分别为 64 天和 20 天。在两名患者中,血细胞计数直到死亡仍未恢复正常。在两名患者中,我们注意到肝酶升高。其中一例在甲型肝炎的愈合期被诊断为丙氨酸转氨酶和天冬氨酸转氨酶 CTC 四级升高。这些值在停止替莫唑胺治疗后恢复正常。一名患者在治疗期间死于肺炎。
我们的生存数据与文献中的数据相当。然而,我们注意到骨髓和肝脏的副作用发生率和强度相当高。这些建议在治疗期间应定期检查血细胞计数和肝酶,并根据制造商给出的标准应用或终止替莫唑胺。