Srinagarind Hospital, Khon Kaen University, Khon Kaen, Thailand.
AIDS Res Ther. 2011 Oct 26;8:40. doi: 10.1186/1742-6405-8-40.
There are limited data of immunologic and virologic failure in Asian HIV-infected children using non-nucleoside reverse transcriptase inhibitor (NNRTI)-based highly active antiretroviral therapy (HAART). We examined the incidence rate of immunologic failure (IF) and virologic failure (VF) and the accuracy of using IF to predict VF in Thai HIV-infected children using first-line NNRTI-based HAART.
Antiretroviral (ART)-naïve HIV-infected children from 2 prospective cohorts treated with NNRTI-based HAART during 2001-2008 were included. CD4 counts were performed every 12 weeks and plasma HIV-RNA measured every 24 weeks. Immune recovery was defined as CD4%≥25%. IF was defined as persistent decline of ≥5% in CD4% in children with CD4%<15% at baseline or decrease in CD4 count ≥30% from baseline. VF was defined as HIV-RNA>1,000 copies/ml after at least 24 weeks of HAART. Clinical and laboratory parameter changes were assessed using a paired t-test, and a time to event approach was used to assess predictors of VF. Sensitivity and specificity of IF were calculated against VF.
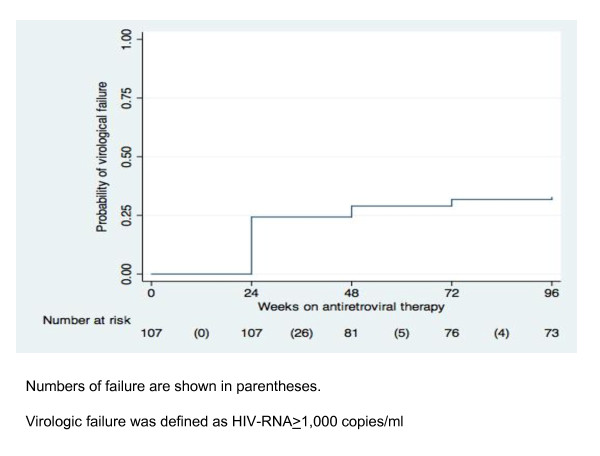
107 ART-naive HIV-infected children were included, 52% female, % CDC clinical classification N:A:B:C 4:44:30:22%. Baseline data were median (IQR) age 6.2 (4.2-8.9) years, CD4% 7 (3-15), HIV-RNA 5.0 (4.9-5.5) log10copies/ml. Nevirapine (NVP) and efavirenz (EFV)-based HAART were started in 70% and 30%, respectively.At 96 weeks, none had progressed to a CDC clinical classification of AIDS and one had died from pneumonia. Overall, significant improvement of weight for age z-score (p = 0.014), height for age z-score, hemoglobin, and CD4 were seen (all p < 0.001). The median (IQR) CD4% at 96 weeks was 25 (18-30)%. Eighty-nine percent of children had immune recovery (CD4%≥25%) and 75% of children had HIV-RNA <1.7log10copies/ml.Thirty five (32.7%) children experienced VF within 96 weeks. Of these, 24 (68.6%) and 31 (88.6%) children had VF in the first 24 and 48 weeks respectively.Only 1 (0.9%) child experienced IF within 96 weeks and the sensitivity (95%CI) of IF to VF was 4 (0.1-20.4)% and specificity was 100 (93.9-100)%.
Immunologic failure, as defined here, had low sensitivity compared to VF and should not be recommended to detect treatment failure. Plasma HIV-RNA should be performed twice, at weeks 24 and 48, to detect early treatment failure.
Clinicaltrials.gov identification number NCT00476606.
使用非核苷类逆转录酶抑制剂(NNRTI)为基础的高效抗逆转录病毒治疗(HAART)的亚洲 HIV 感染儿童的免疫和病毒学失败数据有限。我们检查了免疫失败(IF)和病毒学失败(VF)的发生率,以及使用 IF 预测泰国 HIV 感染儿童使用一线 NNRTI 为基础的 HAART 的 VF 的准确性。
纳入了来自 2 个前瞻性队列的抗逆转录病毒(ART)初治 HIV 感染儿童,他们在 2001-2008 年期间接受了 NNRTI 为基础的 HAART 治疗。每 12 周进行一次 CD4 计数,每 24 周测量一次血浆 HIV-RNA。免疫恢复定义为 CD4%≥25%。IF 定义为基线时 CD4%<15%的儿童中 CD4%持续下降≥5%,或从基线下降≥30%。VF 定义为 HAART 至少 24 周后 HIV-RNA>1,000 拷贝/ml。使用配对 t 检验评估临床和实验室参数变化,使用时间事件方法评估 VF 的预测因素。计算 IF 对 VF 的敏感性和特异性。
纳入了 107 名 ART 初治 HIV 感染儿童,52%为女性,%CDC 临床分类 N:A:B:C 为 4:44:30:22%。基线数据中位数(IQR)为年龄 6.2(4.2-8.9)岁,CD4%为 7(3-15),HIV-RNA 为 5.0(4.9-5.5)log10copies/ml。Nevirapine(NVP)和依非韦伦(EFV)为基础的 HAART 分别开始于 70%和 30%的患者。96 周时,无一例进展为 CDC 临床分类 AIDS,一例死于肺炎。总体而言,体重年龄 z 评分(p=0.014)、身高年龄 z 评分、血红蛋白和 CD4 均有显著改善(均 p<0.001)。96 周时的中位数(IQR)CD4%为 25(18-30)%。89%的儿童有免疫恢复(CD4%≥25%),75%的儿童 HIV-RNA<1.7log10copies/ml。35(32.7%)名儿童在 96 周内发生了 VF。其中,24 名(68.6%)和 31 名(88.6%)儿童分别在第 24 和 48 周出现了 VF。只有 1 名(0.9%)儿童在 96 周内出现 IF,IF 对 VF 的敏感性(95%CI)为 4(0.1-20.4)%,特异性为 100(93.9-100)%。
这里定义的免疫失败与 VF 相比敏感性较低,不建议用于检测治疗失败。应在第 24 和 48 周进行两次血浆 HIV-RNA 检测,以早期发现治疗失败。
Clinicaltrials.gov 编号 NCT00476606。