The Centre for Medication Safety and Service Quality, The School of Pharmacy, Tavistock Square, UK.
BMC Med Res Methodol. 2011 Nov 3;11:149. doi: 10.1186/1471-2288-11-149.
There is a recognised need to build primary care medication adherence services which are tailored to patients' needs. Continuous quality improvement of such services requires a regular working method of measuring adherence in order to monitor effectiveness. Self report has been considered the method of choice for clinical use; it is cheap, relatively unobtrusive and able to distinguish between intentional and unintentional non-adherence, which have different underlying causes and therefore require different interventions. A self report adherence measure used in routine clinical practice would ideally be brief, acceptable to patients, valid, reliable, have the ability to distinguish between different types of non-adherence and be able to be completed by or in conjunction with carers where necessary.
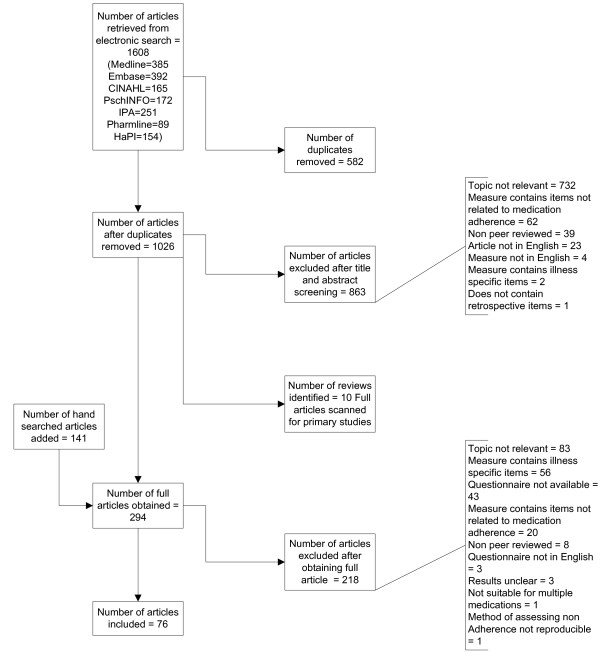
We systematically reviewed the literature in order to identify self report adherence measures currently available which are suitable for primary care and evaluate the extent to which they met the criteria described above. We searched the databases Medline, Embase, International Pharmaceutical Abstracts, Pharmline, CINAHL, PsycINFO and HaPI to identify studies reporting the development, validation or reliability of generic adherence measures. One reviewer screened all abstracts and assessed all relevant full text articles obtained and a second reviewer screened/assessed 10% to check reliability.
Fifty eight measures were identified. While validation data were presented in support of the vast majority of self reported measures (54/58), data for a relatively small number of measures was presented for reliability (16/58) and time to complete (3/58). Few were designed to have the ability to be completed by or in conjunction with carers and few were able to distinguish between different types of non-adherence, which limited their ability be used effectively in the continuous improvement of targeted adherence enhancing interventions. The data available suggested that patients find it easier to estimate general adherence than to report a specific number of doses missed. Visual analogue scales can be easier for patients than other types of scale but are not suitable for telephone administration.
There is a need for a measure which can be used in the routine continual quality monitoring of adherence services.
需要建立针对患者需求定制的初级保健药物依从性服务,以提高医疗质量。此类服务的持续质量改进需要定期使用测量药物依从性的工作方法,以监测其有效性。自我报告被认为是临床应用的首选方法;它便宜、相对不引人注目,能够区分有意和无意的不依从,因为这两者具有不同的潜在原因,因此需要不同的干预措施。在常规临床实践中使用的自我报告依从性测量方法,理想情况下应该简短、患者易于接受、有效、可靠、能够区分不同类型的不依从,并能够在必要时由或与护理人员一起完成。
我们系统地审查了文献,以确定目前适用于初级保健的自我报告依从性测量方法,并评估它们在多大程度上符合上述标准。我们在 Medline、Embase、International Pharmaceutical Abstracts、Pharmline、CINAHL、PsycINFO 和 HaPI 数据库中进行了检索,以确定报告通用依从性测量方法的开发、验证或可靠性的研究。一位评审员筛选了所有摘要,并评估了获得的所有相关全文文章,第二位评审员筛选/评估了 10%的文章以检查可靠性。
确定了 58 项措施。虽然验证数据支持了绝大多数自我报告的措施(54/58),但只有相对较少的措施(16/58)提供了可靠性数据,还有 3/58 提供了完成时间数据。很少有措施旨在能够由或与护理人员一起完成,很少有措施能够区分不同类型的不依从,这限制了它们在有针对性的增强药物依从性干预措施的持续改进中有效使用的能力。现有数据表明,患者发现估计总体依从性比报告特定的漏服剂量更容易。视觉模拟量表比其他类型的量表更适合患者,但不适合电话管理。
需要有一种能够用于常规持续监测依从性服务的测量方法。