Knapik Piotr, Ciesla Daniel, Borowik Dawid, Czempik Piotr, Knapik Tomasz
Department of Cardiac Anaesthesia and Intensive Care, Silesian Centre for Heart Diseases, Zabrze, Poland.
J Cardiothorac Surg. 2011 Nov 23;6:158. doi: 10.1186/1749-8090-6-158.
Few available models aim to identify patients at risk of prolonged ventilation after cardiac surgery. We compared prediction models developed in ICU in two adjacent periods of time, when significant changes were observed both in population characteristics and the perioperative management.
We performed a retrospective review of two cohorts of patients in our department in two subsequent time periods (July 2007 - December 2008, n = 2165; January 2009 - July 2010, n = 2192). The study was approved by the Institutional Ethics Committee and the individual patient consent was not required. Patients were divided with regard to ventilation time of more or less than 48 hours. Preoperative and procedure-related variables for prolonged ventilation were identified and multivariate logistic regression analysis was performed separately for each cohort.
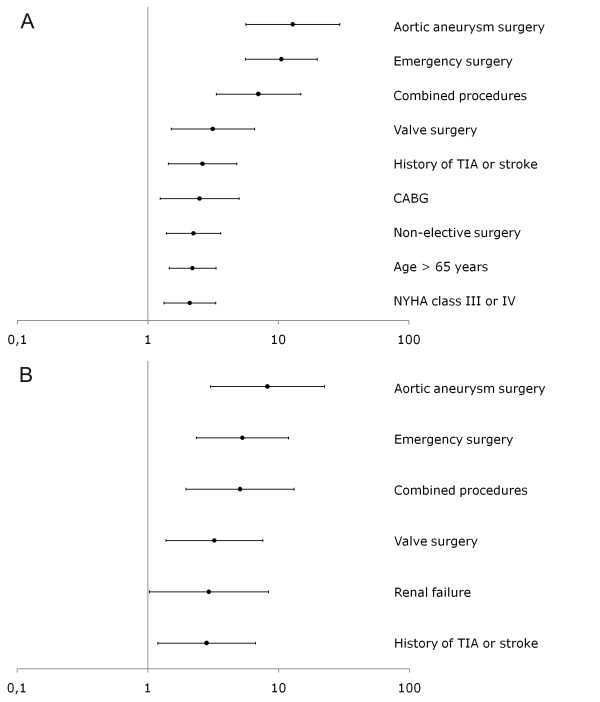
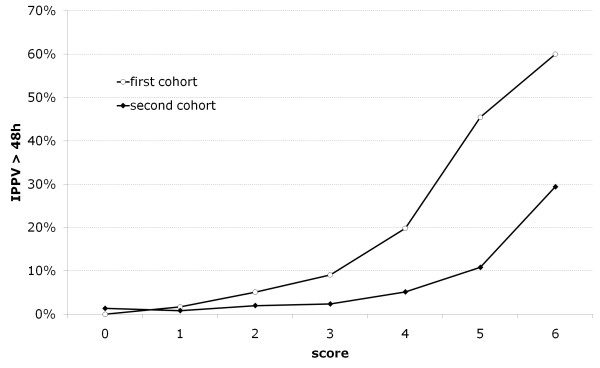
Most recent patients were older, with more co-morbidities, more frequently undergoing off-pump surgery. At the beginning of 2009 we also changed the technique of postoperative ventilation. Percentage of patients with prolonged ventilation decreased from 5.7% to 2.4% (p < 0.0001). Preoperative and procedure-related variables for prolonged ventilation were identified. Prediction models for prolonged ventilation were different for each cohort. Most recent significant predictors were: aortic aneurysm surgery (OR 12.9), emergency surgery (OR 5.3), combined procedures (OR 5.1), valve procedures (OR 3.2), preoperative renal dysfunction (OR 2.9) and preoperative stroke or TIA (OR 2.8).
Prediction models for postoperative ventilation should be regularly updated, particularly when major changes are noted in patients' demographics and surgical or anaesthetic technique.
目前很少有模型旨在识别心脏手术后有长时间通气风险的患者。我们比较了在重症监护病房(ICU)两个相邻时间段开发的预测模型,这两个时间段在患者特征和围手术期管理方面均观察到显著变化。
我们对本部门两个连续时间段(2007年7月至2008年12月,n = 2165;2009年1月至2010年7月,n = 2192)的两组患者进行了回顾性研究。该研究经机构伦理委员会批准,无需患者个人同意。根据通气时间是否超过48小时对患者进行分组。确定了与长时间通气相关的术前和手术相关变量,并对每个队列分别进行多因素逻辑回归分析。
最近的患者年龄更大,合并症更多,更频繁地接受非体外循环手术。2009年初我们还改变了术后通气技术。长时间通气患者的比例从5.7%降至2.4%(p < 0.0001)。确定了与长时间通气相关的术前和手术相关变量。每个队列的长时间通气预测模型不同。最近的显著预测因素为:主动脉瘤手术(比值比[OR] 12.9)、急诊手术(OR 5.3)、联合手术(OR 5.1)、瓣膜手术(OR 3.2)、术前肾功能不全(OR 2.9)和术前中风或短暂性脑缺血发作(TIA)(OR 2.8)。
术后通气的预测模型应定期更新,尤其是在患者人口统计学特征以及手术或麻醉技术出现重大变化时。