Herrin Jeph, Miller Lauren E, Turkmani Dima F, Nsa Wato, Drye Elizabeth E, Bernheim Susannah M, Ling Shari M, Rapp Michael T, Han Lein F, Bratzler Dale W, Bradley Elizabeth H, Nallamothu Brahmajee K, Ting Henry H, Krumholz Harlan M
Section of Cardiovascular Medicine, Department of Internal Medicine, Yale University School of Medicine, New Haven, Connecticut, USA.
Arch Intern Med. 2011 Nov 28;171(21):1879-86. doi: 10.1001/archinternmed.2011.481.
Delays in treatment time are commonplace for patients with ST-segment elevation acute myocardial infarction who must be transferred to another hospital for percutaneous coronary intervention. Experts have recommended that door-in to door-out (DIDO) time (ie, time from arrival at the first hospital to transfer from that hospital to the percutaneous coronary intervention hospital) should not exceed 30 minutes. We sought to describe national performance in DIDO time using a new measure developed by the Centers for Medicare & Medicaid Services.
We report national median DIDO time and examine associations with patient characteristics (age, sex, race, contraindication to fibrinolytic therapy, and arrival time) and hospital characteristics (number of beds, geographic region, location [rural or urban], and number of cases reported) using a mixed effects multivariable model.
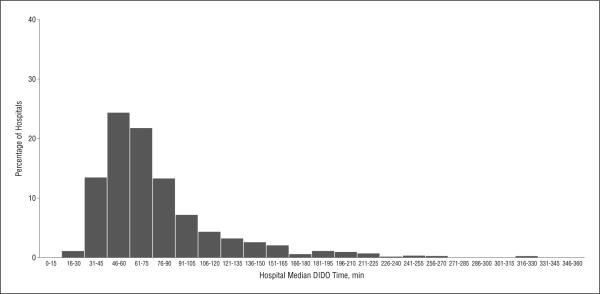
Among 13,776 included patients from 1034 hospitals, only 1343 (9.7%) had a DIDO time within 30 minutes, and DIDO exceeded 90 minutes for 4267 patients (31.0%). Mean estimated times (95% CI) to transfer based on multivariable analysis were 8.9 (5.6-12.2) minutes longer for women, 9.1 (2.7-16.0) minutes longer for African Americans, 6.9 (1.6-11.9) minutes longer for patients with contraindication to fibrinolytic therapy, shorter for all age categories (except >75 years) relative to the category of 18 to 35 years, 15.3 (7.3-23.5) minutes longer for rural hospitals, and 14.4 (6.6-21.3) minutes longer for hospitals with 9 or fewer transfers vs 15 or more in 2009 (all P < .001).
Among patients presenting to emergency departments and requiring transfer to another facility for percutaneous coronary intervention, the DIDO time rarely met the recommended 30 minutes.
对于必须转至另一家医院进行经皮冠状动脉介入治疗的ST段抬高型急性心肌梗死患者,治疗时间延迟很常见。专家建议,门到门(DIDO)时间(即从抵达第一家医院到从该医院转至经皮冠状动脉介入治疗医院的时间)不应超过30分钟。我们试图使用医疗保险和医疗补助服务中心开发的一项新指标来描述全国在DIDO时间方面的表现。
我们报告全国DIDO时间中位数,并使用混合效应多变量模型研究其与患者特征(年龄、性别、种族、溶栓治疗禁忌证及到达时间)和医院特征(床位数、地理区域、位置[农村或城市]及报告病例数)之间的关联。
在来自1034家医院的13776例纳入患者中,只有1343例(9.7%)的DIDO时间在30分钟以内,4267例患者(31.0%)的DIDO时间超过90分钟。基于多变量分析的平均估计转院时间(95%CI)显示,女性长8.9(5.6 - 12.2)分钟,非裔美国人长9.1(2.7 - 16.0)分钟,有溶栓治疗禁忌证的患者长6.9(1.6 - 11.9)分钟,相对于18至35岁年龄组,所有其他年龄组(75岁以上除外)转院时间较短,农村医院长15.3(7.3 - 23.5)分钟,2009年转院9例或更少的医院比转院15例或更多的医院长14.4(6.6 - 21.3)分钟(所有P <.001)。
在就诊于急诊科且需转至另一家机构进行经皮冠状动脉介入治疗的患者中,DIDO时间很少能达到推荐的30分钟。