Division of Human Genetics, The Children's Hospital of Philadelphia, Philadelphia, Pennsylvania, USA.
Am J Med Genet B Neuropsychiatr Genet. 2012 Jan;159B(1):87-93. doi: 10.1002/ajmg.b.32005. Epub 2011 Dec 13.
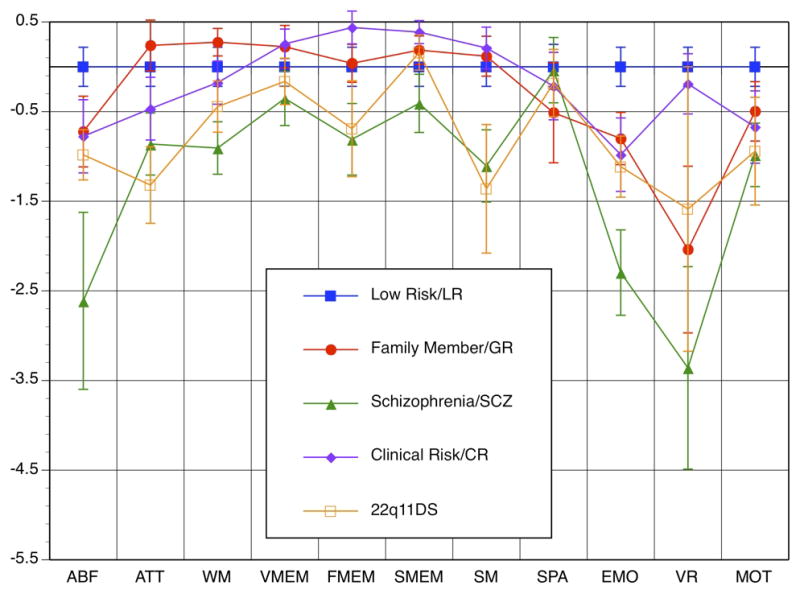
Adults with 22q11.2 Deletion syndrome (22q11DS) have increased prevalence of schizophrenia features. Our goal is to compare the neurocognitive profile in 22q11DS, schizophrenia and individuals at risk for schizophrenia. Twenty-one 22q11DS patients (8-32 years, mean 14.9 years, 15M, 6F) were matched to four comparison groups on age: low risk (n = 21), first-degree family members of schizophrenia patients (genetic risk, n = 20), individuals exhibiting putatively prodromal symptoms (clinical risk, n = 19), and patients with schizophrenia (n = 21). All participants received semi-structured interviews [Diagnostic Interview for Genetic Studies (DIGS) and the Structured Interview for Prodromal Syndromes (SIPS)], and a computerized neurocognitive battery (CNB) measuring the following domains: Abstraction and Mental Flexibility, Attention, Working Memory, Verbal Memory, Face Memory, Spatial Memory, Language, Spatial Processing, Sensorimotor Dexterity, and Emotion Processing. Sixty percent of 22q11DS participants met SIPS criteria for prodromal symptoms and one participant met criteria for paranoid schizophrenia. Thirty-eight percent met criteria for Depressive Disorders. All 22q11DS participants successfully completed the CNB. 22q11DS participants were significantly less accurate in nearly all domains, but had similar speed of response compared to the other groups. Their profile resembled that of the psychosis groups in accuracy and speed, except for more pronounced deficits in accuracy for face memory and emotion processing. Subthreshold psychotic symptoms are present in a high proportion of 22q11DS participants. Deficits shown in the CNB are more pronounced for accuracy than speed relative to the psychosis groups with similar profiles. Similar deficits have been described in the 22q11DS population using non-computerized measures, which require increased testing time.
22q11.2 缺失综合征(22q11DS)患者的精神分裂症特征患病率增加。我们的目标是比较 22q11DS、精神分裂症和精神分裂症高危个体的神经认知特征。21 例 22q11DS 患者(8-32 岁,平均 14.9 岁,15 名男性,6 名女性)按年龄与 4 个对照组相匹配:低危组(n=21)、精神分裂症患者一级亲属(遗传风险,n=20)、表现出前驱症状的个体(临床风险,n=19)和精神分裂症患者(n=21)。所有参与者均接受半结构化访谈[遗传研究诊断访谈(DIGS)和前驱症状结构化访谈(SIPS)]和计算机化神经认知测试(CNB),测试以下领域:抽象思维和思维灵活性、注意力、工作记忆、言语记忆、面孔记忆、空间记忆、语言、空间处理、感觉运动灵巧、情绪处理。60%的 22q11DS 患者符合前驱症状 SIPS 标准,1 名患者符合偏执型精神分裂症标准。38%的患者符合抑郁障碍标准。所有 22q11DS 患者均成功完成 CNB。22q11DS 患者在几乎所有领域的准确性都明显较低,但与其他组的反应速度相似。他们的表现与精神病组在准确性和速度上相似,除了面孔记忆和情绪处理的准确性缺陷更为明显。亚阈值精神病症状在 22q11DS 患者中比例较高。与具有相似特征的精神病组相比,CNB 中的缺陷在准确性上比速度上更为明显。使用非计算机化测量方法在 22q11DS 人群中也描述了类似的缺陷,这些方法需要更长的测试时间。