Gur R E, Yi J J, McDonald-McGinn D M, Tang S X, Calkins M E, Whinna D, Souders M C, Savitt A, Zackai E H, Moberg P J, Emanuel B S, Gur R C
Department of Psychiatry, Neuropsychiatry Section, Prelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA.
1] Department of Psychiatry, Neuropsychiatry Section, Prelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA [2] Department of Child and Adolescent Psychiatry, Children's Hospital of Philadelphia, Philadelphia, PA, USA.
Mol Psychiatry. 2014 Nov;19(11):1205-11. doi: 10.1038/mp.2013.189. Epub 2014 Jan 21.
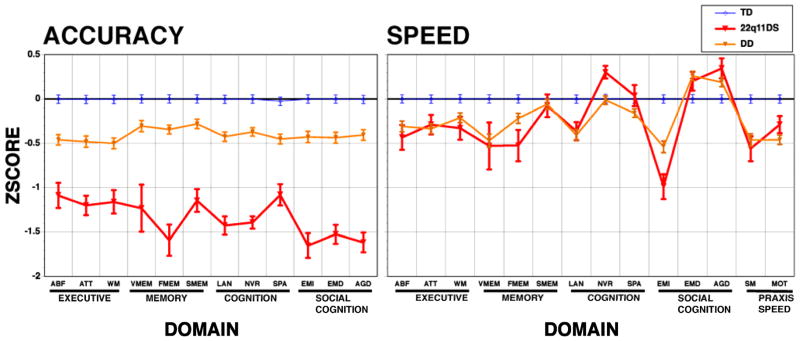
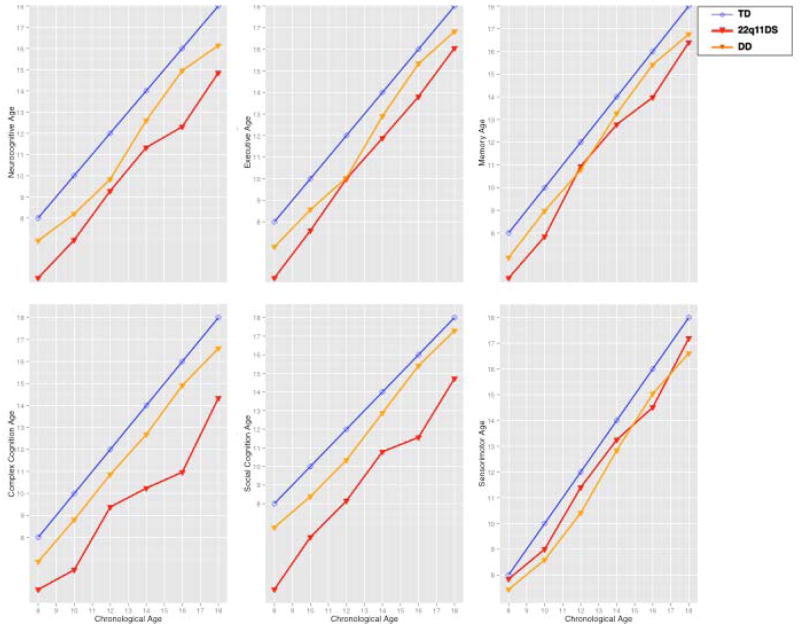
The 22q11.2 deletion syndrome (22q11DS) presents with medical and neuropsychiatric manifestations including neurocognitive deficits. Quantitative neurobehavioral measures linked to brain circuitry can help elucidate genetic mechanisms contributing to deficits. To establish the neurocognitive profile and neurocognitive 'growth charts', we compared cross-sectionally 137 individuals with 22q11DS ages 8-21 to 439 demographically matched non-deleted individuals with developmental delay (DD) and medical comorbidities and 443 typically developing (TD) participants. We administered a computerized neurocognitive battery that measures performance accuracy and speed in executive, episodic memory, complex cognition, social cognition and sensorimotor domains. The accuracy performance profile of 22q11DS showed greater impairment than DD, who were impaired relative to TD. Deficits in 22q11DS were most pronounced for face memory and social cognition, followed by complex cognition. Performance speed was similar for 22q11DS and DD, but 22q11DS individuals were differentially slower in face memory and emotion identification. The growth chart, comparing neurocognitive age based on performance relative to chronological age, indicated that 22q11DS participants lagged behind both groups from the earliest age assessed. The lag ranged from less than 1 year to over 3 years depending on chronological age and neurocognitive domain. The greatest developmental lag across the age range was for social cognition and complex cognition, with the smallest for episodic memory and sensorimotor speed, where lags were similar to DD. The results suggest that 22q11.2 microdeletion confers specific vulnerability that may underlie brain circuitry associated with deficits in several neuropsychiatric disorders, and therefore help identify potential targets and developmental epochs optimal for intervention.
22q11.2缺失综合征(22q11DS)会出现包括神经认知缺陷在内的医学和神经精神症状。与脑回路相关的定量神经行为测量有助于阐明导致缺陷的遗传机制。为了建立神经认知概况和神经认知“生长图表”,我们对137名年龄在8至21岁的22q11DS个体与439名在人口统计学上匹配的有发育迟缓(DD)和医学合并症的非缺失个体以及443名发育正常(TD)的参与者进行了横断面比较。我们使用了一个计算机化神经认知测试组合,测量执行、情景记忆、复杂认知、社会认知和感觉运动领域的表现准确性和速度。22q11DS的准确性表现概况显示出比DD更严重的损伤,而DD相对于TD也有损伤。22q11DS在面部记忆和社会认知方面的缺陷最为明显,其次是复杂认知。22q11DS和DD的表现速度相似,但22q11DS个体在面部记忆和情绪识别方面的速度差异更大。根据表现相对于实际年龄的神经认知年龄比较得出的生长图表表明,22q11DS参与者从最早评估的年龄起就落后于两组。根据实际年龄和神经认知领域的不同,落后时间从不到1年到超过3年不等。在整个年龄范围内,社会认知和复杂认知的发育滞后最大,情景记忆和感觉运动速度的滞后最小,后者的滞后与DD相似。结果表明,22q11.2微缺失赋予了特定的易损性,这可能是与几种神经精神疾病缺陷相关的脑回路基础,因此有助于确定潜在的干预靶点和最佳发育时期。