Demoruelle M Kristen, Weisman Michael H, Simonian Philip L, Lynch David A, Sachs Peter B, Pedraza Isabel F, Harrington Annie R, Kolfenbach Jason R, Striebich Christopher C, Pham Quyen N, Strickland Colin D, Petersen Brian D, Parish Mark C, Derber Lezlie A, Norris Jill M, Holers V Michael, Deane Kevin D
University of Colorado, Aurora, CO, USA.
Arthritis Rheum. 2012 Jun;64(6):1756-61. doi: 10.1002/art.34344. Epub 2011 Dec 19.
To evaluate the presence of pulmonary abnormalities in rheumatoid arthritis (RA)-related autoantibody-positive subjects without inflammatory arthritis.
Forty-two subjects who did not have inflammatory arthritis but were positive for anti-cyclic citrullinated peptide antibodies and/or ≥2 rheumatoid factor isotypes (a profile that is 96% specific for RA), 15 autoantibody-negative controls, and 12 patients with established seropositive early RA (<1-year duration) underwent spirometry and high-resolution computed tomography (HRCT) lung imaging.
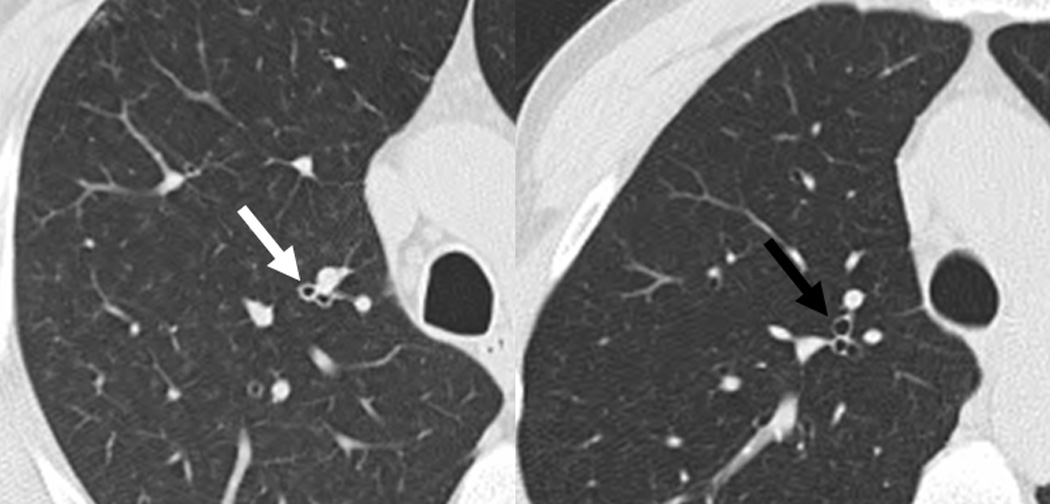
The median age of autoantibody-positive subjects was 54 years, 52% were female, and 38% were ever-smokers; these characteristics were not significantly different from those of autoantibody-negative control subjects. No autoantibody-positive subject had inflammatory arthritis based on joint examination. HRCT revealed that 76% of autoantibody-positive subjects had airways abnormalities including bronchial wall thickening, bronchiectasis, centrilobular opacities, and air trapping, compared with 33% of autoantibody-negative controls (P = 0.005). The prevalence and type of lung abnormalities among autoantibody-positive subjects were similar to those among patients with early RA. In 2 autoantibody-positive subjects with airways disease, inflammatory arthritis classifiable as articular RA developed ∼13 months after the lung evaluation.
Airways abnormalities that are consistent with inflammation are common in autoantibody-positive subjects without inflammatory arthritis and are similar to airways abnormalities seen in patients with early RA. These findings suggest that the lung may be an early site of autoimmune-related injury and potentially a site of generation of RA-related autoimmunity. Further studies are needed to define the mechanistic role of lung inflammation in the development of RA.
评估无炎性关节炎的类风湿关节炎(RA)相关自身抗体阳性受试者肺部异常情况。
42名无炎性关节炎但抗环瓜氨酸肽抗体和/或≥2种类风湿因子亚型呈阳性(该特征对RA的特异性为96%)的受试者、15名自身抗体阴性对照者以及12名确诊的血清阳性早期RA患者(病程<1年)接受了肺功能测定和高分辨率计算机断层扫描(HRCT)肺部成像检查。
自身抗体阳性受试者的中位年龄为54岁,52%为女性,38%为曾经吸烟者;这些特征与自身抗体阴性对照者无显著差异。根据关节检查,无自身抗体阳性受试者患有炎性关节炎。HRCT显示,76%的自身抗体阳性受试者存在气道异常,包括支气管壁增厚、支气管扩张、小叶中心性混浊和空气潴留,而自身抗体阴性对照者中这一比例为33%(P = 0.005)。自身抗体阳性受试者肺部异常的患病率和类型与早期RA患者相似。在2名患有气道疾病的自身抗体阳性受试者中,可归类为关节型RA的炎性关节炎在肺部评估后约13个月出现。
与炎症一致的气道异常在无炎性关节炎的自身抗体阳性受试者中很常见,且与早期RA患者所见的气道异常相似。这些发现表明,肺可能是自身免疫相关损伤的早期部位,也可能是RA相关自身免疫产生的部位。需要进一步研究来确定肺部炎症在RA发病机制中的作用。