Tri-Institutional MD-PhD Program, Weill Cornell Medical College/The Rockefeller University/Sloan-Kettering Cancer Institute, New York, NY 10021, USA.
J Mol Cell Cardiol. 2012 Mar;52(3):608-19. doi: 10.1016/j.yjmcc.2011.12.003. Epub 2011 Dec 16.
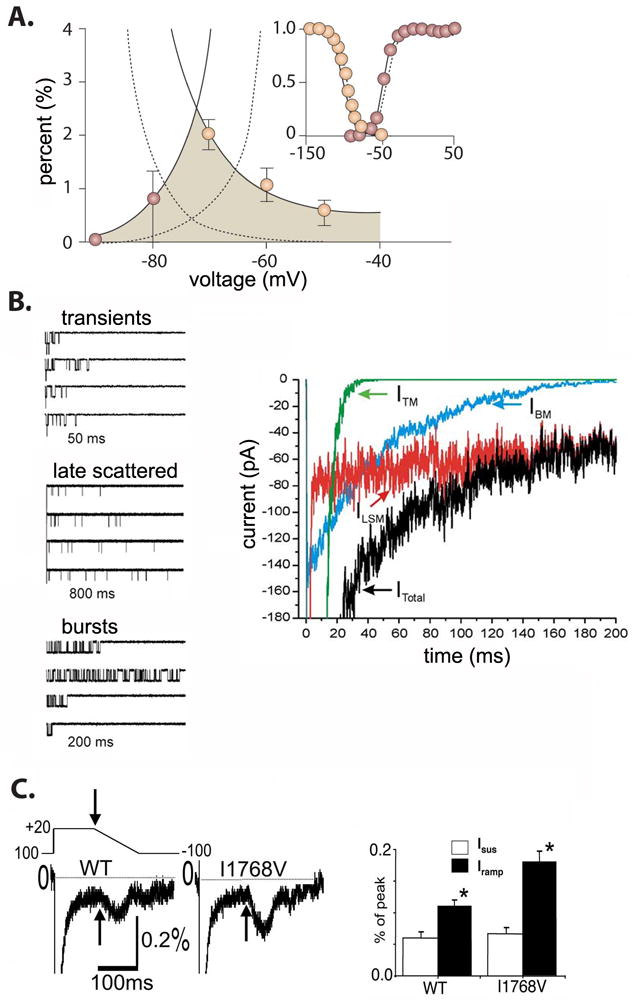
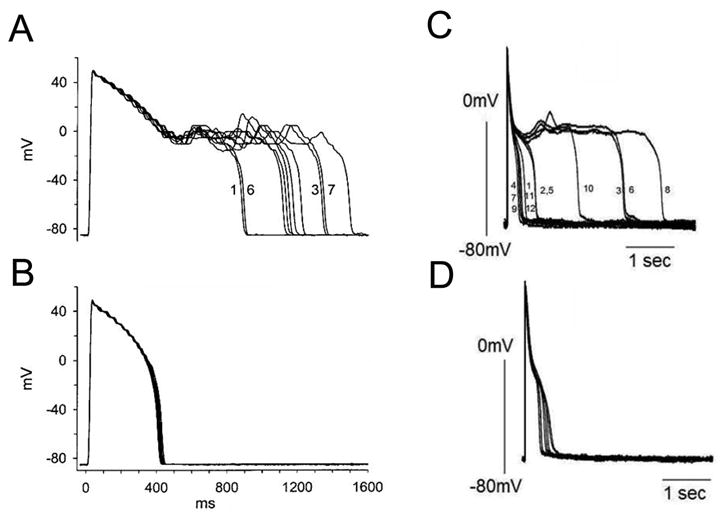
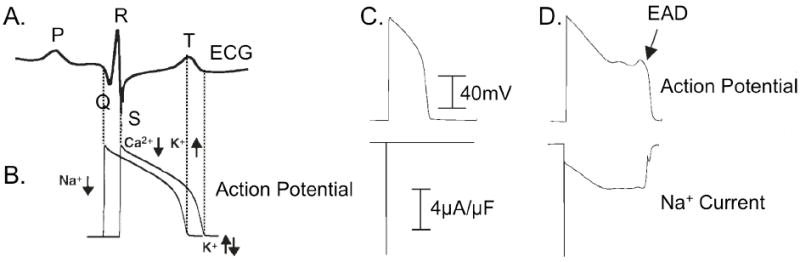
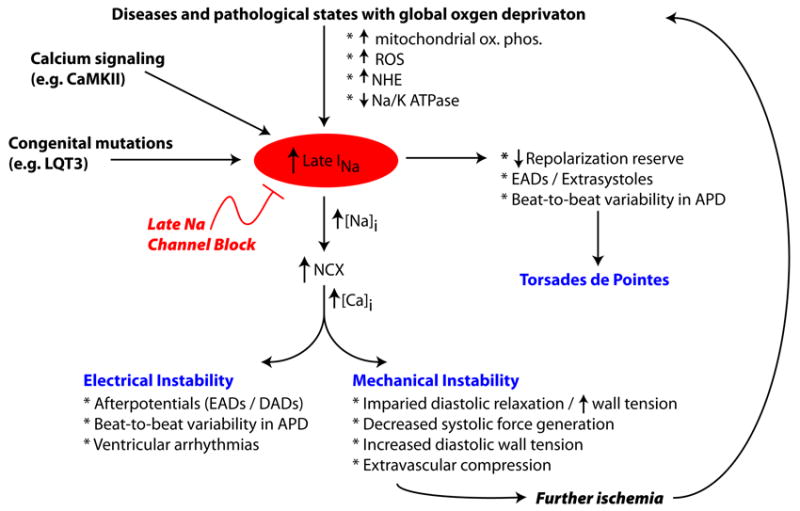
A pathological increase in the late component of the cardiac Na(+) current, I(NaL), has been linked to disease manifestation in inherited and acquired cardiac diseases including the long QT variant 3 (LQT3) syndrome and heart failure. Disruption in I(NaL) leads to action potential prolongation, disruption of normal cellular repolarization, development of arrhythmia triggers, and propensity to ventricular arrhythmia. Attempts to treat arrhythmogenic sequelae from inherited and acquired syndromes pharmacologically with common Na(+) channel blockers (e.g. flecainide, lidocaine, and amiodarone) have been largely unsuccessful. This is due to drug toxicity and the failure of most current drugs to discriminate between the peak current component, chiefly responsible for single cell excitability and propagation in coupled tissue, and the late component (I(NaL)) of the Na(+) current. Although small in magnitude as compared to the peak Na(+) current (~1-3%), I(NaL) alters action potential properties and increases Na(+) loading in cardiac cells. With the increasing recognition that multiple cardiac pathological conditions share phenotypic manifestations of I(NaL) upregulation, there has been renewed interest in specific pharmacological inhibition of I(Na). The novel antianginal agent ranolazine, which shows a marked selectivity for late versus peak Na(+) current, may represent a novel drug archetype for targeted reduction of I(NaL). This article aims to review common pathophysiological mechanisms leading to enhanced I(NaL) in LQT3 and heart failure as prototypical disease conditions. Also reviewed are promising therapeutic strategies tailored to alter the molecular mechanisms underlying I(Na) mediated arrhythmia triggers.
心脏钠电流晚期成分(I(NaL))病理性增加与遗传性和获得性心脏病的疾病表现有关,包括长 QT 变异 3 型(LQT3)综合征和心力衰竭。I(NaL)的中断会导致动作电位延长、正常细胞复极化中断、心律失常触发因素的发展以及室性心律失常的倾向。尝试使用常见的钠通道阻滞剂(例如氟卡尼、利多卡因和胺碘酮)从遗传性和获得性综合征中通过药理学方法治疗心律失常的后果在很大程度上是不成功的。这是由于药物毒性和大多数当前药物无法区分主要负责单细胞兴奋性和耦合组织中传播的峰电流分量与钠电流的晚期分量(I(NaL))。尽管与峰钠电流(~1-3%)相比,I(NaL)的幅度较小,但它会改变动作电位特性并增加心脏细胞中的钠负荷。随着越来越多的人认识到多种心脏病理状况具有 I(NaL)上调的表型表现,人们对特定的 I(Na)药理学抑制重新产生了兴趣。新型抗心绞痛药物雷诺嗪对晚期与峰值钠电流具有明显的选择性,可能代表针对 I(NaL)靶向减少的新型药物原型。本文旨在综述导致 LQT3 和心力衰竭等典型疾病条件下 I(NaL)增强的常见病理生理机制。还回顾了针对改变 I(Na)介导的心律失常触发的分子机制的有前途的治疗策略。