Department of Obstetrics and Gynaecology, Kenyatta National Hospital/University of Nairobi, Kenya.
J Int AIDS Soc. 2011 Dec 28;14:61. doi: 10.1186/1758-2652-14-61.
We set out to determine the relative roles of stigma versus health systems in non-uptake of prevention of mother to child transmission (PMTCT) of HIV-1 interventions: we conducted cross-sectional assessment of all consenting mothers accompanying infants for six-week immunizations.
Between September 2008 and March 2009, mothers at six maternal and child health clinics in Kenya's Nairobi and Nyanza provinces were interviewed regarding PMTCT intervention uptake during recent pregnancy. Stigma was ascertained using a previously published standardized questionnaire and infant HIV-1 status determined by HIV-1 polymerase chain reaction.
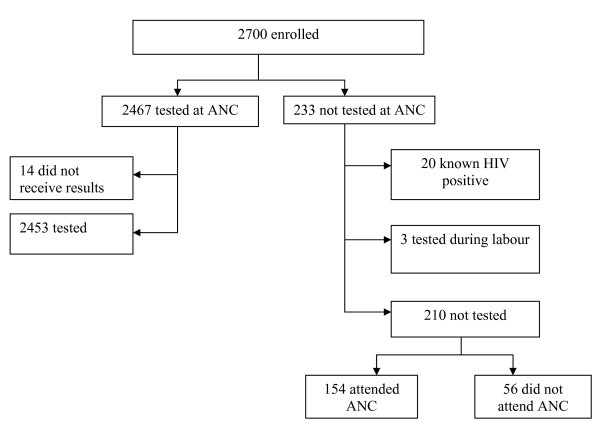
Among 2663 mothers, 2453 (92.1%) reported antenatal HIV-1 testing. Untested mothers were more likely to have less than secondary education (85.2% vs. 74.9%, p=0.001), be from Nyanza (47.1% vs. 32.2%, p<0.001) and have lower socio-economic status. Among 318 HIV-1-infected mothers, 90% reported use of maternal or infant antiretrovirals. Facility delivery was less common among HIV-1-infected mothers (69% vs. 76%, p=0.009) and was associated with antiretroviral use (p<0.001). Although internal or external stigma indicators were reported by between 12% and 59% of women, stigma was not associated with lower HIV-1 testing or infant HIV-1 infection rates; internal stigma was associated with modestly decreased antiretroviral uptake. Health system factors contributed to about 60% of non-testing among mothers who attended antenatal clinics and to missed opportunities in offering antiretrovirals and utilization of facility delivery. Eight percent of six-week-old HIV-1-exposed infants were HIV-1 infected.
Antenatal HIV-1 testing and antiretroviral uptake was high (both more than 90%) and infant HIV-1 infection risk was low, reflecting high PMTCT coverage. Investment in health systems to deliver HIV-1 testing and antiretrovirals can effectively prevent infant HIV-1 infection despite substantial HIV-1 stigma.
我们旨在确定污名与卫生系统在预防母婴传播(PMTCT)艾滋病毒 1 干预措施方面的相对作用:我们对在肯尼亚内罗毕和纳安萨省六个母婴健康诊所陪同婴儿进行六周免疫接种的所有同意母亲进行了横断面评估。使用以前发表的标准化问卷来确定污名,并用 HIV-1 聚合酶链反应来确定婴儿 HIV-1 状态。
2008 年 9 月至 2009 年 3 月,在肯尼亚内罗毕和纳安萨省的六个母婴健康诊所,对 2663 名母亲进行了采访,询问了她们最近怀孕期间接受 PMTCT 干预措施的情况。使用以前发表的标准化问卷来确定污名,并用 HIV-1 聚合酶链反应来确定婴儿 HIV-1 状态。
在 2663 名母亲中,2453 名(92.1%)报告了产前 HIV-1 检测。未接受检测的母亲更有可能受教育程度较低(85.2%对 74.9%,p=0.001),来自纳安萨(47.1%对 32.2%,p<0.001),社会经济地位较低。在 318 名 HIV-1 感染的母亲中,90%报告使用了母婴抗逆转录病毒药物。HIV-1 感染母亲的分娩场所较少(69%对 76%,p=0.009),并且与抗逆转录病毒的使用相关(p<0.001)。尽管有 12%至 59%的女性报告存在内部或外部污名指标,但污名与较低的 HIV-1 检测率或婴儿 HIV-1 感染率无关;内部污名与抗逆转录病毒使用率略有下降有关。卫生系统因素导致在参加产前诊所的母亲中约有 60%未进行 HIV-1 检测,并导致错过了提供抗逆转录病毒药物的机会和利用分娩场所的机会。8%的六周大的 HIV-1 暴露婴儿感染了 HIV-1。
产前 HIV-1 检测和抗逆转录病毒药物的使用率很高(均超过 90%),婴儿 HIV-1 感染风险很低,反映出 PMTCT 的高覆盖率。尽管存在大量 HIV-1 污名,但对卫生系统进行投资以提供 HIV-1 检测和抗逆转录病毒药物,可以有效地预防婴儿 HIV-1 感染。