All India Institute of Medical Sciences, Delhi, India.
PLoS One. 2012;7(1):e29129. doi: 10.1371/journal.pone.0029129. Epub 2012 Jan 3.
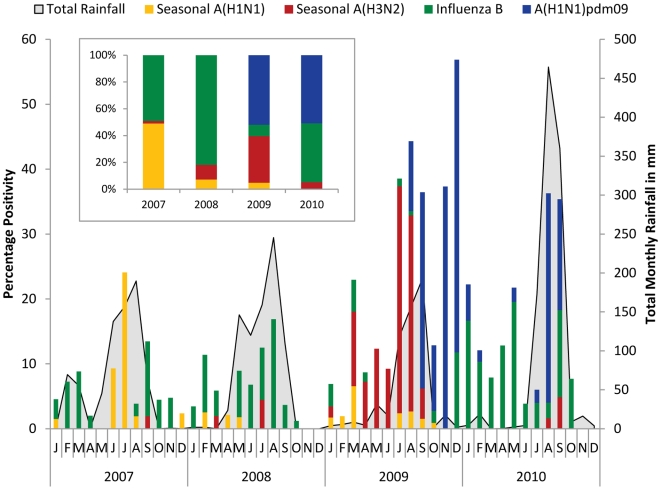
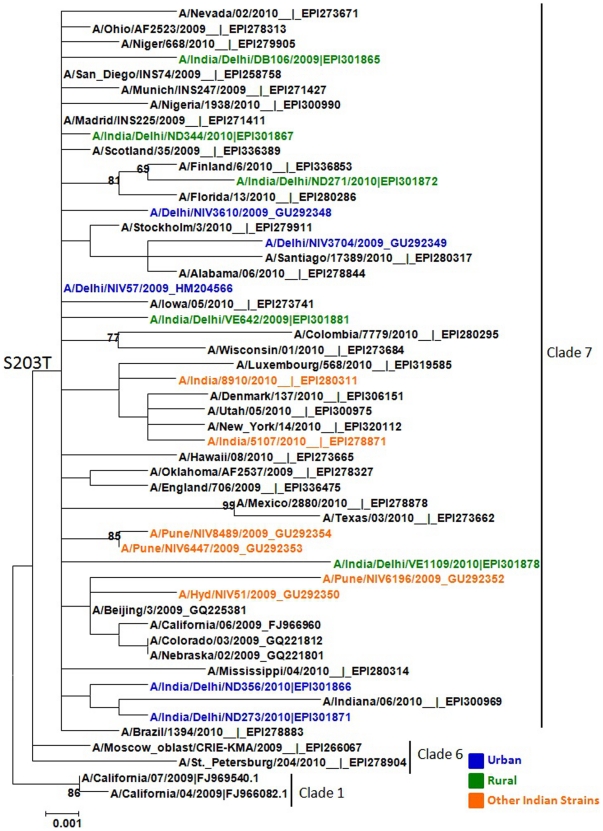
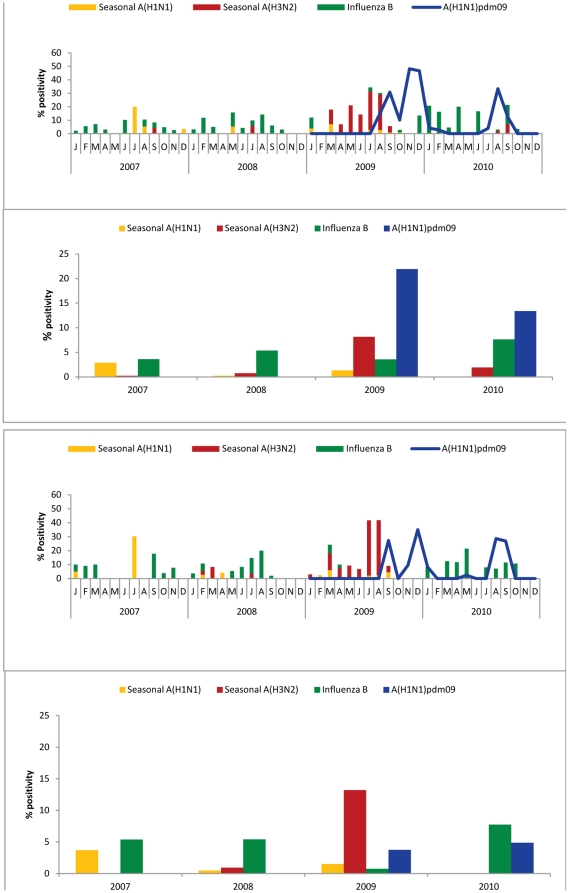
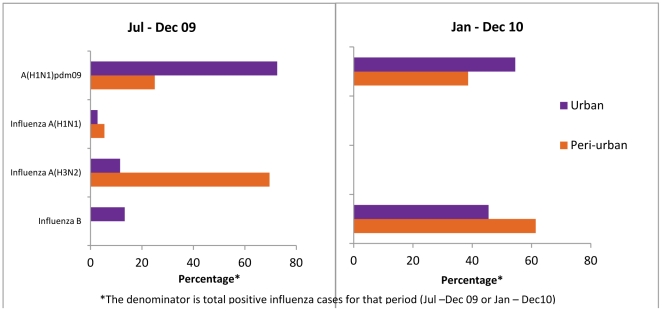
Influenza surveillance was carried out in a subset of patients with influenza-like illness (ILI) presenting at an Employee Health Clinic (EHS) at All India Institute of Medical Sciences (AIIMS), New Delhi (urban) and pediatric out patients department of civil hospital at Ballabhgarh (peri-urban), under the Comprehensive Rural Health Services Project (CRHSP) of AIIMS, in Delhi region from January 2007 to December 2010. Of the 3264 samples tested, 541 (17%) were positive for influenza viruses, of which 221 (41%) were pandemic Influenza A(H1N1)pdm09, 168 (31%) were seasonal influenza A, and 152 (28%) were influenza B. While the Influenza viruses were detected year-round, their types/subtypes varied remarkably. While there was an equal distribution of seasonal A(H1N1) and influenza B in 2007, predominance of influenza B was observed in 2008. At the beginning of 2009, circulation of influenza A(H3N2) viruses was observed, followed later by emergence of Influenza A(H1N1)pdm09 with co-circulation of influenza B viruses. Influenza B was dominant subtype in early 2010, with second wave of Influenza A(H1N1)pdm09 in August-September, 2010. With the exception of pandemic H1N1 emergence in 2009, the peaks of influenza activity coincided primarily with monsoon season, followed by minor peak in winter at both urban and rural sites. Age group analysis of influenza positivity revealed that the percent positivity of Influenza A(H1N1)pdm09 influenza virus was highest in >5-18 years age groups (OR 2.5; CI = 1.2-5.0; p = 0.009) when compared to seasonal influenza. Phylogenetic analysis of Influenza A(H1N1)pdm09 from urban and rural sites did not reveal any major divergence from other Indian strains or viruses circulating worldwide. Continued surveillance globally will help define regional differences in influenza seasonality, as well as, to determine optimal periods to implement influenza vaccination programs among priority populations.
2007 年 1 月至 2010 年 12 月,在全印医学科学研究所(AIIMS)下属的综合农村卫生服务项目(CRHSP)下,在新德里(城市)的员工健康诊所(EHS)和巴拉尔加尔(城郊)的公立医院儿科门诊对患有流感样疾病(ILI)的患者进行了流感监测。在检测的 3264 个样本中,有 541 个(17%)流感病毒检测呈阳性,其中 221 个(41%)为大流行性甲型 H1N1pdm09,168 个(31%)为季节性甲型流感,152 个(28%)为乙型流感。虽然流感病毒全年都有检测到,但它们的类型/亚型差异显著。虽然 2007 年季节性 H1N1 和乙型流感的分布相等,但 2008 年乙型流感占主导地位。2009 年初,观察到甲型 H3N2 病毒的传播,随后甲型 H1N1pdm09 病毒的出现与乙型流感病毒的共同传播。2010 年初乙型流感是主要的亚型,2010 年 8 月至 9 月出现第二波甲型 H1N1pdm09 流感。除了 2009 年大流行 H1N1 的出现外,流感活动的高峰期主要与季风季节相吻合,随后在城市和农村地区的冬季出现小高峰。流感阳性的年龄组分析显示,与季节性流感相比,甲型 H1N1pdm09 流感病毒在>5-18 岁年龄组的阳性率最高(比值比 2.5;95%置信区间 1.2-5.0;p=0.009)。对城乡地区甲型 H1N1pdm09 的系统发育分析显示,与全球流行的其他印度株或病毒相比,没有发现任何重大差异。全球持续监测将有助于确定流感季节性的地区差异,并确定在优先人群中实施流感疫苗接种计划的最佳时期。