Duke University Medical Center, 2301 Erwin Road, 5693 HAFS Bldg., DUMC 3094 Durham, NC 27710, USA.
Anesth Analg. 2012 Mar;114(3):533-46. doi: 10.1213/ANE.0b013e31823ee030. Epub 2012 Jan 17.
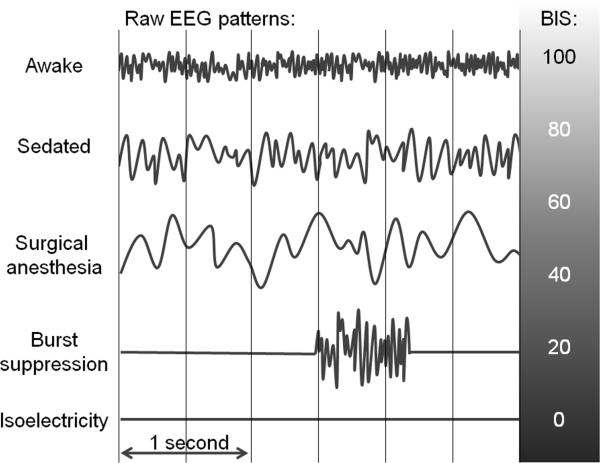
Cardiac surgery presents particular challenges for the anesthesiologist. In addition to standard and advanced monitors typically used during cardiac surgery, anesthesiologists may consider monitoring the brain with raw or processed electroencephalography (EEG). There is strong evidence that a protocol incorporating the processed EEG bispectral index (BIS) decreases the incidence intraoperative awareness in comparison with standard practice. However, there is conflicting evidence that incorporating the BIS into cardiac anesthesia practice improves "fast-tracking," decreases anesthetic drug use, or detects cerebral ischemia. Recent research, including many cardiac surgical patients, shows that a protocol based on BIS monitoring is not superior to a protocol based on end-tidal anesthetic concentration monitoring in preventing awareness. There has been a resurgence of interest in the anesthesia literature in limited montage EEG monitoring, including nonproprietary processed indices. This has been accompanied by research showing that with structured training, anesthesiologists can glean useful information from the raw EEG trace. In this review, we discuss both the hypothesized benefits and limitations of BIS and frontal channel EEG monitoring in the cardiac surgical population.
心脏手术对麻醉师提出了特殊的挑战。除了心脏手术中通常使用的标准和高级监测器外,麻醉师可能还会考虑使用原始或处理后的脑电图 (EEG) 监测大脑。有强有力的证据表明,与标准实践相比,包含处理后 EEG 双频谱指数 (BIS) 的方案可降低术中意识的发生率。然而,有相互矛盾的证据表明,将 BIS 纳入心脏麻醉实践可改善“快速通道”,减少麻醉药物使用或检测脑缺血。最近的研究包括许多心脏手术患者,表明基于 BIS 监测的方案并不优于基于呼气末麻醉浓度监测的方案,无法预防意识。麻醉文献中对有限导联 EEG 监测(包括非专利处理指数)的兴趣重新兴起。这伴随着研究表明,通过结构化培训,麻醉师可以从原始 EEG 迹线上获取有用的信息。在这篇综述中,我们讨论了 BIS 和额通道 EEG 监测在心脏手术人群中的假设益处和局限性。