University of Wuerzburg, Institute of Virology und Immunobiology, 97078 Wuerzburg, Germany.
BMC Infect Dis. 2012 Jan 20;12:14. doi: 10.1186/1471-2334-12-14.
HIV-associated general immune activation is a strong predictor for HIV disease progression, suggesting that chronic immune activation may drive HIV pathogenesis. Consequently, immunomodulating agents may decelerate HIV disease progression.
In an observational study, we determined immune activation in HIV patients receiving low-dose (5 mg/day) prednisolone with or without highly-active antiretroviral therapy (HAART) compared to patients without prednisolone treatment. Lymphocyte activation was determined by flow cytometry detecting expression of CD38 on CD8(+) T cells. The monocyte activation markers sCD14 and LPS binding protein (LBP) as well as inflammation markers soluble urokinase plasminogen activated receptor (suPAR) and sCD40L were determined from plasma by ELISA.
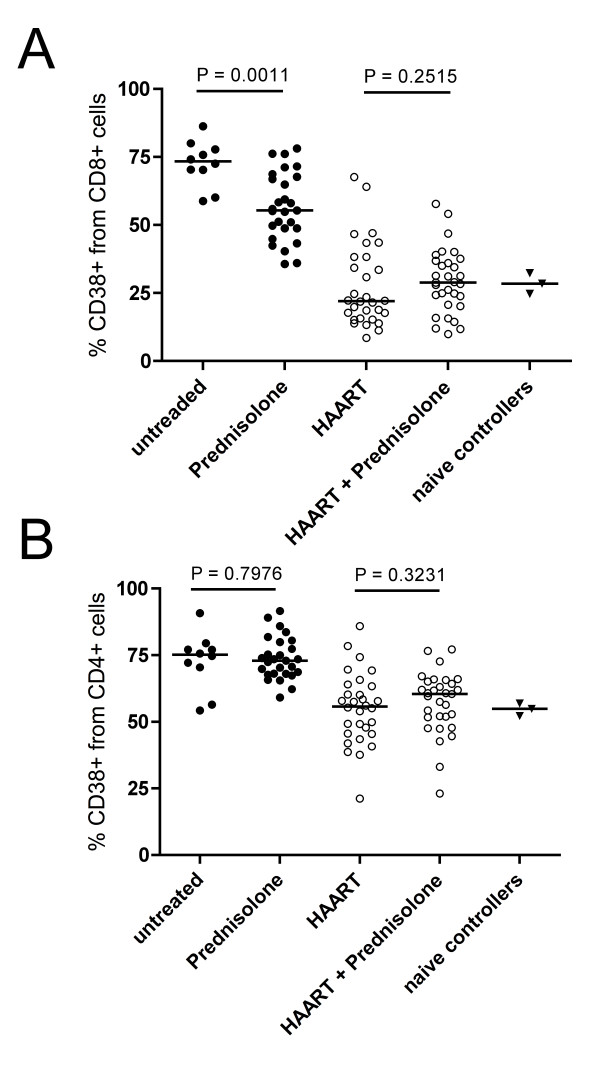
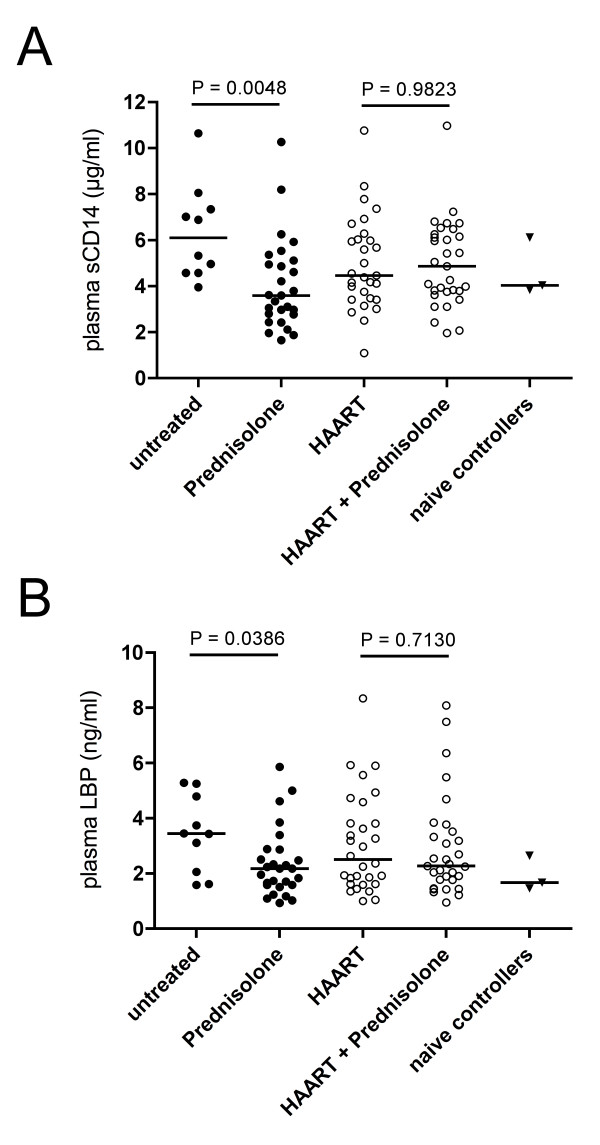
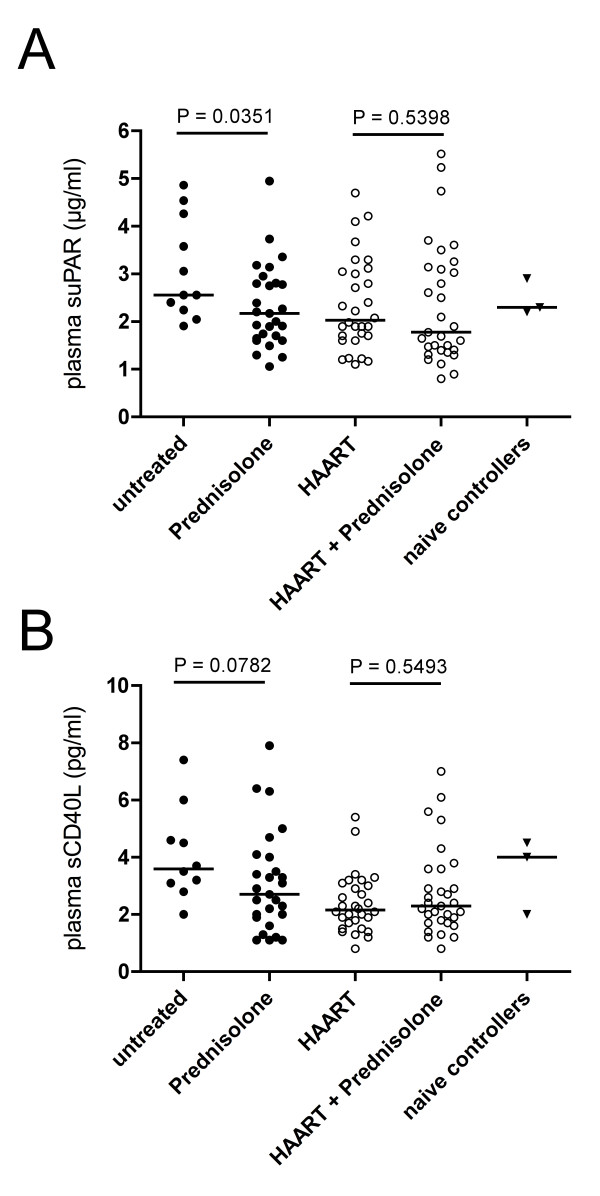
CD38-expression on CD8+ T lymphocytes was significantly lower in prednisolone-treated patients compared to untreated patients (median 55.40% [percentile range 48.76-67.70] versus 73.34% [65.21-78.92], p = 0.0011, Mann-Whitney test). Similarly, we detected lower levels of sCD14 (3.6 μg/ml [2.78-5.12] vs. 6.11 μg/ml [4.58-7.70]; p = 0.0048), LBP (2.18 ng/ml [1.59-2.87] vs. 3.45 ng/ml [1.84-5.03]; p = 0.0386), suPAR antigen (2.17 μg/ml [1.65-2.81] vs. 2.56 μg/ml [2.24-4.26]; p = 0.0351) and a trend towards lower levels of sCD40L (2.70 pg/ml [1.90-4.00] vs. 3.60 pg/ml [2.95-5.30]; p = 0.0782). Viral load in both groups was similar (0.8 × 105 ng/ml [0.2-42.4 × 105] vs. 1.1 × 105 [0.5-12.2 × 105]; p = 0.3806). No effects attributable to prednisolone were observed when patients receiving HAART in combination with prednisolone were compared to patients who received HAART alone.
Patients treated with low-dose prednisolone display significantly lower general immune activation than untreated patients. Further longitudinal studies are required to assess whether treatment with low-dose prednisolone translates into differences in HIV disease progression.
HIV 相关的全身性免疫激活是 HIV 疾病进展的强有力预测指标,这表明慢性免疫激活可能推动 HIV 的发病机制。因此,免疫调节药物可能会减缓 HIV 的疾病进展。
在一项观察性研究中,我们比较了接受低剂量(5mg/天)泼尼松龙联合或不联合高效抗逆转录病毒治疗(HAART)与未接受泼尼松龙治疗的 HIV 患者的免疫激活情况。通过流式细胞术检测 CD8+T 细胞上 CD38 的表达来确定淋巴细胞的激活。通过 ELISA 从血浆中测定单核细胞激活标志物可溶性 CD14(sCD14)和脂多糖结合蛋白(LBP)以及炎症标志物可溶性尿激酶型纤溶酶原激活物受体(suPAR)和 sCD40L。
与未治疗的患者相比,接受泼尼松龙治疗的患者 CD8+T 淋巴细胞上的 CD38 表达明显降低(中位数 55.40%[百分位范围 48.76-67.70] 与 73.34%[65.21-78.92],p=0.0011,Mann-Whitney 检验)。同样,我们检测到 sCD14 水平降低(3.6μg/ml[2.78-5.12]与 6.11μg/ml[4.58-7.70];p=0.0048)、LBP 水平降低(2.18ng/ml[1.59-2.87]与 3.45ng/ml[1.84-5.03];p=0.0386)、suPAR 抗原水平降低(2.17μg/ml[1.65-2.81]与 2.56μg/ml[2.24-4.26];p=0.0351),sCD40L 水平呈降低趋势(2.70pg/ml[1.90-4.00]与 3.60pg/ml[2.95-5.30];p=0.0782)。两组患者的病毒载量相似(0.8×105ng/ml[0.2-42.4×105]与 1.1×105ng/ml[0.5-12.2×105];p=0.3806)。当比较接受 HAART 联合泼尼松龙治疗的患者与仅接受 HAART 治疗的患者时,没有观察到泼尼松龙治疗的作用。
接受低剂量泼尼松龙治疗的患者表现出明显低于未治疗患者的全身性免疫激活。需要进一步的纵向研究来评估低剂量泼尼松龙治疗是否会导致 HIV 疾病进展的差异。