Paganelli G, De Cicco C, Ferrari M E, McVie G, Pagani G, Leonardi M C, Cremonesi M, Ferrari A, Pacifici M, Di Dia A, Botta F, De Santis R, Galimberti V, Luini A, Orecchia R, Veronesi U
Division of Nuclear Medicine.
Ecancermedicalscience. 2010;4:166. doi: 10.3332/ecancer.2010.166. Epub 2010 Nov 1.
Breast conserving surgery (BCS) plus external beam radiotherapy (EBRT) is considered the standard treatment for early breast cancer. We have investigated the possibility of irradiating the residual gland, using an innovative nuclear medicine approach named IART(®) (Intra-operative Avidination for Radionuclide Therapy).
The objective of this study was to determine the optimal dose of avidin with a fixed activity (3.7 GBq) of (90)Y-biotin, in order to provide a boost of 20 Gy, followed by EBRT to the whole breast (WB) at the reduced dose of 40 Gy. Local and systemic toxicity, patient's quality of life, including the cosmetic results after the combined treatment with IART(®) and EBRT, were assessed.
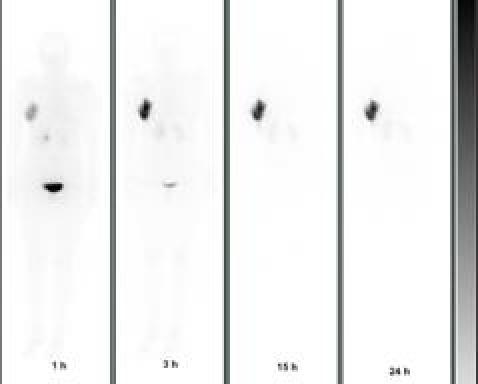
After tumour excision, the surgeon injected native avidin diluted in 30 ml of saline solution into and around the tumour bed (see video). Patients received one of three avidin dose levels: 50 mg (10 pts), 100 mg (15 pts) and 150 mg (10 pts). Between 12 to 24 h after surgery, 3.7 GBq (90)Y-biotin spiked with 185 MBq (111)In-biotin was administered intravenously (i.v.). Whole body scans and SPECT images were performed up to 30 h post-injection for dosimetric purposes. WB-EBRT was administered four weeks after the IART(®) boost. Local toxicity and quality of life were evaluated.
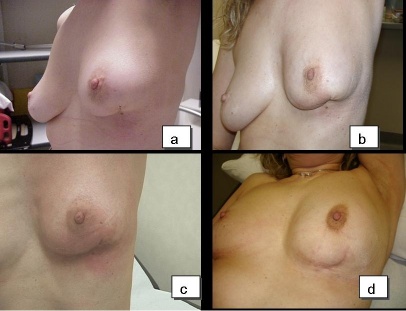
Thirty-five patients were evaluated. No side effects were observed after avidin administration and (90)Y-biotin infusion. An avidin dose level of 100 mg resulted the most appropriate in order to deliver the required radiation dose (19.5 ± 4.0 Gy) to the surgical bed. At the end of IART(®), no local toxicity occurred and the overall cosmetic result was good. The tolerance to the reduced EBRT was also good. The highest grade of transient local toxicity was G3, which occurred in 3/32 pts following the completion of WB-EBRT. The combination of IART(®)+EBRT was well accepted by the patients, without any changes to their quality of life.
These preliminary results support the hypothesis that IART(®) may represent a valid approach to accelerated WB irradiation after BCS. We hope that this nuclear medicine technique will contribute to a better management of breast cancer patients.
保乳手术(BCS)加体外照射放疗(EBRT)被认为是早期乳腺癌的标准治疗方法。我们研究了使用一种名为IART(®)(术中放射性核素治疗的抗生物素蛋白化)的创新核医学方法对残留腺体进行照射的可能性。
本研究的目的是确定在固定活度(3.7 GBq)的(90)Y-生物素情况下抗生物素蛋白的最佳剂量,以便给予20 Gy的增敏剂量,随后以40 Gy的降低剂量对全乳(WB)进行EBRT。评估局部和全身毒性、患者的生活质量,包括IART(®)和EBRT联合治疗后的美容效果。
肿瘤切除后,外科医生将稀释于30 ml盐溶液中的天然抗生物素蛋白注入肿瘤床及其周围(见视频)。患者接受三种抗生物素蛋白剂量水平之一:50 mg(10例)、100 mg(15例)和150 mg(10例)*。在手术后12至24小时之间,静脉注射(i.v.)3.7 GBq(90)Y-生物素加185 MBq(111)In-生物素。为进行剂量测定,在注射后长达30小时进行全身扫描和SPECT图像检查。在IART(®)增敏后四周给予WB-EBRT。评估局部毒性和生活质量。
评估了35例患者。抗生物素蛋白给药和(90)Y-生物素输注后未观察到副作用。100 mg的抗生物素蛋白剂量水平最适合向手术床给予所需的辐射剂量(19.5±4.0 Gy)。在IART(®)结束时,未发生局部毒性,总体美容效果良好。对降低剂量的EBRT的耐受性也良好。最高级别的短暂局部毒性为G3,在WB-EBRT完成后3/32例患者中出现。IART(®)+EBRT的联合治疗被患者很好地接受,他们的生活质量没有任何变化。
这些初步结果支持以下假设,即IART(®)可能是BCS后加速WB照射的一种有效方法。我们希望这种核医学技术将有助于更好地管理乳腺癌患者。
*注:pts为患者(patients)的缩写,翻译时保留英文缩写更符合医学文献习惯。