Department of Emergency Medicine, Carolinas Medical Center, Charlotte, NC, USA.
J Thromb Haemost. 2012 Apr;10(4):572-81. doi: 10.1111/j.1538-7836.2012.04647.x.
Increasing the threshold to define a positive D-dimer could reduce unnecessary computed tomographic pulmonary angiography (CTPA) for a suspected pulmonary embolism (PE) but might increase rates of a missed PE and missed pneumonia, the most common non-thromboembolic diagnosis seen on CTPA.
Measure the effect of doubling the standard D-dimer threshold for 'PE unlikely' Revised Geneva (RGS) or Wells' scores on the exclusion rate, frequency and size of a missed PE and missed pneumonia.
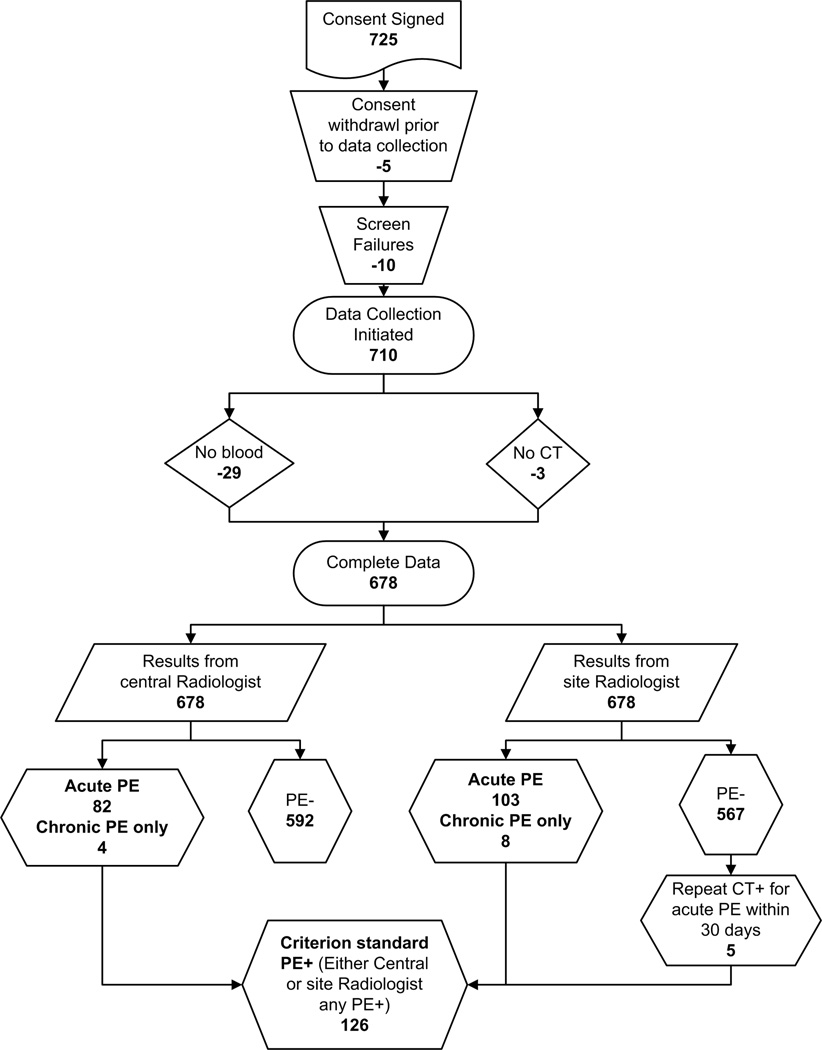
Patients evaluated for a suspected PE with 64-channel CTPA were prospectively enrolled from emergency departments (EDs) and inpatient units of four hospitals. Pretest probability data were collected in real time and the D-dimer was measured in a central laboratory. Criterion standard was CPTA interpretation by two independent radiologists combined with clinical outcome at 30 days.
Of 678 patients enrolled, 126 (19%) were PE+ and 93 (14%) had pneumonia. Use of either Wells' ≤ 4 or RGS ≤ 6 produced similar results. For example, with RGS ≤ 6 and standard threshold (< 500 ng mL(-1)), D-dimer was negative in 110/678 (16%), and 4/110 were PE+ (posterior probability 3.8%) and 9/110 (8.2%) had pneumonia. With RGS ≤ 6 and a threshold < 1000 ng mL(-1) , D-dimer was negative in 208/678 (31%) and 11/208 (5.3%) were PE+, but 10/11 missed PEs were subsegmental and none had concomitant DVT. Pneumonia was found in 12/208 (5.4%) with RGS ≤ 6 and D-dimer < 1000 ng mL(-1).
Doubling the threshold for a positive D-dimer with a PE unlikely pretest probability could reduce CTPA scanning with a slightly increased risk of missed isolated subsegmental PE, and no increase in rate of missed pneumonia.
提高 D-二聚体阳性阈值以诊断可疑肺栓塞(PE),可能会减少不必要的 CT 肺动脉造影(CTPA)检查,但可能会增加漏诊 PE 和肺炎的发生率,而肺炎是 CTPA 最常见的非血栓栓塞性诊断。
测量将修订版日内瓦(RGS)或 Wells 评分中“PE 可能性低”的 D-二聚体标准阈值翻倍对排除率、漏诊 PE 和肺炎的频率和大小的影响。
前瞻性纳入四家医院急诊科和住院部疑似 PE 患者进行 64 排 CTPA 检查。实时收集预测试概率数据,并在中心实验室测量 D-二聚体。将 CTPA 两位独立放射科医生的解读结果与 30 天的临床结局相结合作为金标准。
在纳入的 678 例患者中,126 例(19%)为 PE+,93 例(14%)患有肺炎。使用 Wells≤4 或 RGS≤6 评分得到了相似的结果。例如,在 RGS≤6 和标准阈值(<500ng/mL)下,678 例患者中有 110 例 D-二聚体为阴性(16%),其中 4 例为 PE+(后验概率 3.8%),9 例(8.2%)患有肺炎。在 RGS≤6 和阈值<1000ng/mL 时,678 例患者中有 208 例 D-二聚体为阴性(31%),其中 11 例为 PE+,但 10 例漏诊的 PE 均为亚段性,且均无并发深静脉血栓形成。在 RGS≤6 和 D-二聚体<1000ng/mL 时,208 例患者中有 12 例(5.4%)患有肺炎。
对于 PE 可能性低的患者,将 D-二聚体阳性阈值翻倍,可减少 CTPA 扫描,但可能会略微增加漏诊孤立性亚段性 PE 的风险,且不会增加漏诊肺炎的发生率。