Department of Internal Medicine, Nephrology, University Hospitals Leuven, Herestraat 49, Leuven, B-3000, Belgium.
Crit Care. 2012 Feb 3;16(1):R20. doi: 10.1186/cc11180.
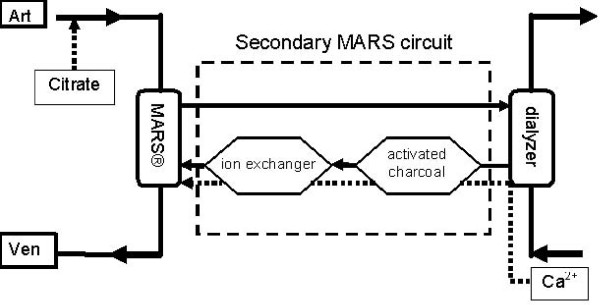
The Molecular Adsorbent Recycling System (MARS) is used to treat patients with liver failure. Observational data suggest that citrate anticoagulation during MARS is feasible. Comparative studies on the optimal anticoagulation regimen during MARS are lacking. The aim of the current study was to evaluate two heparin-free anticoagulation regimens.
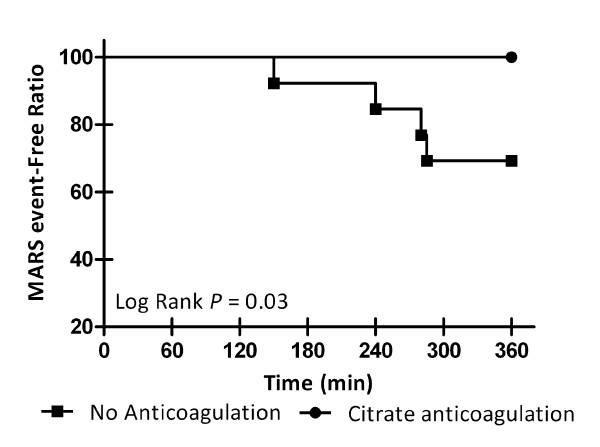
We performed a prospective randomized open-label crossover study of regional citrate anticoagulation against no anticoagulation. Ten patients (age 55±11 years) with liver failure undergoing MARS treatment were included. The primary endpoint was completion of MARS sessions. Secondary endpoints included treatment efficacy and safety. Longevity of MARS treatment was plotted as a Kaplan-Meier estimate. Fisher's exact test was used for contingency table analysis.
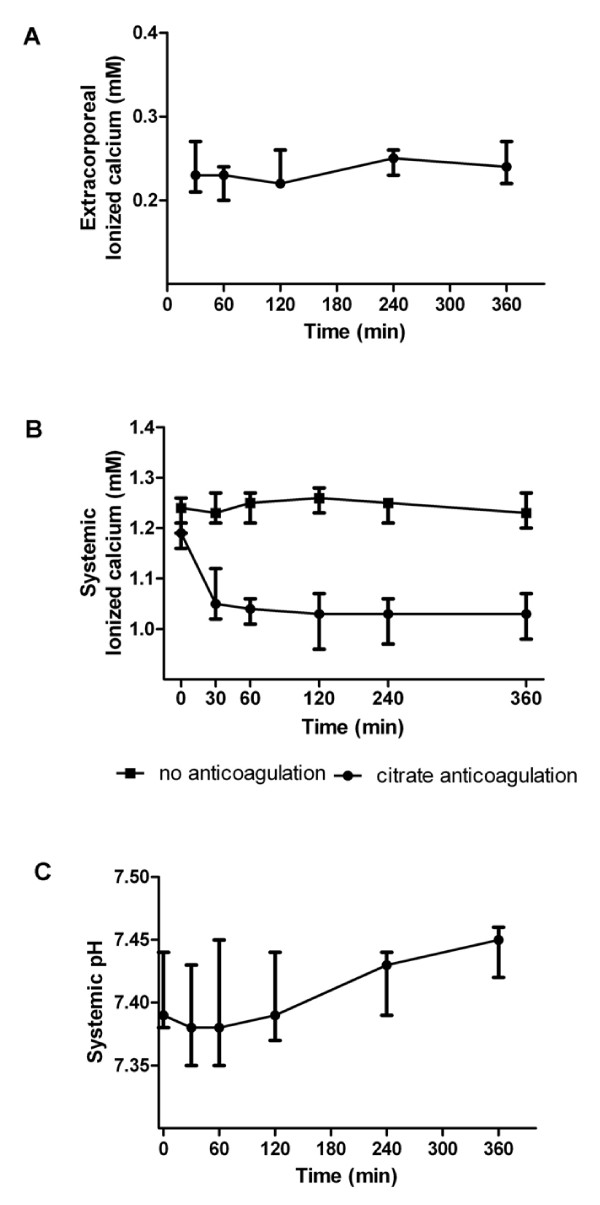
Of a total of 27 6-hour sessions, four sessions had to be terminated prematurely, three due to occlusive clotting of the extracorporeal circuit and one due to uncontrollable bleeding from the vascular access site. All four events occurred in the group without anticoagulation. Between group comparison demonstrated citrate anticoagulation to significantly increase the likelihood of completed MARS treatment (Fisher's exact test, P 0.04). This translates into higher bilirubin reduction ratios when citrate was applied (reduction ratio 0.25 vs. 0.15, P 0.02). Systemic ionized calcium concentrations were significantly reduced during citrate anticoagulation (P<0.001) but remained within a safe range. We observed no major adverse events.
Regional citrate anticoagulation in patients with liver failure is feasible. Citrate anticoagulation provides superior patency of the extracorporeal circuit. Avoidance of anticoagulation during MARS results in significant loss of treatment efficacy, due to treatment downtime. Additional studies are required to identify the optimal anticoagulation regimen for extracorporeal circulation in patients with liver failure.
分子吸附再循环系统(MARS)用于治疗肝功能衰竭患者。观察性数据表明,MARS 期间使用柠檬酸盐抗凝是可行的。缺乏关于 MARS 期间最佳抗凝方案的比较研究。本研究旨在评估两种无肝素抗凝方案。
我们进行了一项前瞻性随机开放标签交叉研究,比较了局部柠檬酸盐抗凝与无抗凝的效果。纳入 10 名(年龄 55±11 岁)肝功能衰竭行 MARS 治疗的患者。主要终点是 MARS 疗程的完成情况。次要终点包括治疗效果和安全性。MARS 治疗的寿命用 Kaplan-Meier 估计绘制。使用 Fisher 确切检验进行列联表分析。
在总共 27 个 6 小时疗程中,有 4 个疗程不得不提前终止,其中 3 个由于体外回路闭塞性血栓形成,1 个由于血管通路部位无法控制的出血。所有 4 个事件均发生在无抗凝组。组间比较表明柠檬酸盐抗凝显著增加了 MARS 治疗完成的可能性(Fisher 确切检验,P=0.04)。这转化为应用柠檬酸盐时胆红素降低率更高(降低率 0.25 对 0.15,P=0.02)。柠檬酸盐抗凝时,系统离子钙浓度显著降低(P<0.001),但仍在安全范围内。我们未观察到重大不良事件。
肝功能衰竭患者局部柠檬酸盐抗凝是可行的。柠檬酸盐抗凝可提供更好的体外回路通畅性。由于治疗停机时间,MARS 期间避免抗凝会导致治疗效果显著丧失。需要进一步研究以确定肝功能衰竭患者体外循环的最佳抗凝方案。