Department of Cardiology, Austin Health, Heidelberg, VIC, Australia.
Cardiovasc Diabetol. 2012 Feb 14;11:14. doi: 10.1186/1475-2840-11-14.
The prognostic benefits of beta-blockers (BB) in patients with systolic heart failure (SHF) are known but despite this, in patients with diabetes they are underutilized. The aim of this study was to assess the effect of beta-blockers (BB) on glycaemic control in patients with Type 2 Diabetes (T2DM) and systolic heart failure (SHF) stratified to beta-1 selective (Bisoprolol) vs. nonselective BB (Carvedilol).
This observational, cohort study was conducted in patients with T2DM and SHF attending an Australian tertiary teaching hospital's heart failure services. The primary endpoint was glycaemic control measured by glycosylated haemoglobin (HbA1c) at initiation and top dose of BB. Secondary endpoints included microalbuminuria, changes in lipid profile and estimated glomerular filtration rate (eGFR).
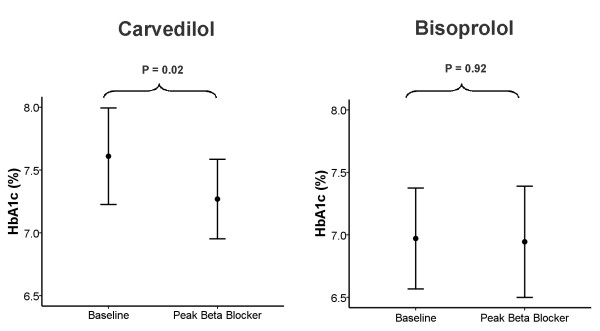
125 patients were assessed. Both groups were well matched for gender, NYHA class and use of guideline validated heart failure and diabetic medications. The mean treatment duration was 1.9 ± 1.1 years with carvedilol and 1.4 ± 1.0 years with bisoprolol (p = ns). The carvedilol group achieved a reduction in HbA1c (7.8 ± 0.21% to 7.3 ± 0.17%, p = 0.02) whereas the bisoprolol group showed no change in HbA1c (7.0 ± 0.20% to 6.9 ± 0.23%, p = 0.92). There was no significant difference in the change in HbA1c from baseline to peak BB dose in the carvedilol group compared to the bisoprolol group. There was a similar deterioration in eGFR, but no significant changes in lipid profile or microalbuminuria in both groups (p = ns).
BB use did not worsen glycaemic control, lipid profile or albuminuria status in subjects with SHF and T2DM. Carvedilol significantly improved glycemic control in subjects with SHF and T2DM and this improvement was non significantly better than that obtained with bisoprolol. BB's should not be withheld from patients with T2DM and SHF.
β 受体阻滞剂(BB)在收缩性心力衰竭(SHF)患者中的预后获益已得到证实,但尽管如此,在患有糖尿病的患者中,它们的使用仍不足。本研究旨在评估β受体阻滞剂(BB)对 2 型糖尿病(T2DM)和收缩性心力衰竭(SHF)患者血糖控制的影响,并对β-1 选择性(比索洛尔)与非选择性 BB(卡维地洛)进行分层。
本观察性队列研究在澳大利亚一家三级教学医院的心力衰竭服务中心就诊的 T2DM 和 SHF 患者中进行。主要终点是通过糖化血红蛋白(HbA1c)在开始和 BB 最大剂量时测量的血糖控制。次要终点包括微量白蛋白尿、血脂谱变化和估算肾小球滤过率(eGFR)。
共评估了 125 例患者。两组在性别、NYHA 分级以及指南验证的心力衰竭和糖尿病药物的使用方面均匹配良好。卡维地洛组的平均治疗持续时间为 1.9 ± 1.1 年,比索洛尔组为 1.4 ± 1.0 年(p = ns)。卡维地洛组的 HbA1c 降低(7.8 ± 0.21%降至 7.3 ± 0.17%,p = 0.02),而比索洛尔组的 HbA1c 无变化(7.0 ± 0.20%降至 6.9 ± 0.23%,p = 0.92)。与比索洛尔组相比,卡维地洛组从基线到 BB 最大剂量的 HbA1c 变化无显著差异。两组的 eGFR 均有类似的恶化,但血脂谱或微量白蛋白尿无显著变化(p = ns)。
在患有 SHF 和 T2DM 的患者中,BB 的使用不会导致血糖控制、血脂谱或白蛋白尿状况恶化。卡维地洛可显著改善 SHF 和 T2DM 患者的血糖控制,且这种改善与比索洛尔相比无显著差异。因此,不应拒绝为患有 T2DM 和 SHF 的患者使用 BB。