State Key Laboratory of Oncology in South China, Department of Radiation Oncology, Sun Yat-sen University Cancer Center, No,651 Dongfeng Road East, Guangzhou 510060, People's Republic of China.
BMC Cancer. 2012 Feb 15;12:68. doi: 10.1186/1471-2407-12-68.
Intensity-modulated radiation therapy (IMRT) provides excellent locoregional control for nasopharyngeal carcinoma (NPC), and has gradually replaced two-dimensional conventional radiotherapy as the first-line radiotherapy technique. Furthermore, in the new seventh edition of the American Joint Committee on Cancer (AJCC) staging system, retropharyngeal lymph nodes were upgraded from N0 to N1 disease as a result of their negative impact on the distant metastasis-free survival (DMFS) rates of NPC. This retrospective study was conducted in order to review the treatment outcomes and patterns of failure in NPC patients with N0 disease after IMRT in order to effectively guide treatment in the future.
We retrospectively reviewed data from 506 biopsy-proven nonmetastatic NPC patients. There were 191 patients with negative cervical lymph node involvement. According to the seventh edition of the American Joint Committee on Cancer (AJCC) staging system, 110 patients (21.7%) were staged with N0 disease, and 81 patients (16.0%) were reclassified with N1 disease due to the presence of RLN metastasis. All patients received IMRT as the primary treatment.
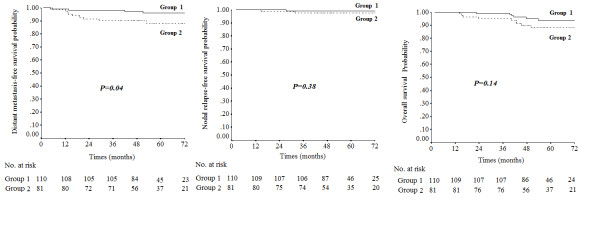
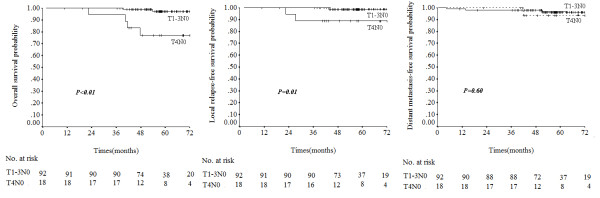
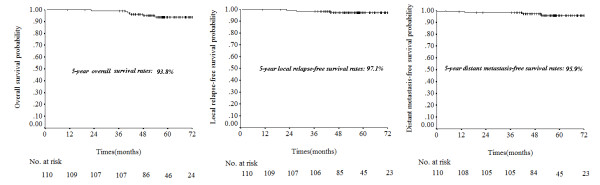
In patients with negative cervical lymph node involvement, distant metastasis-free survival (DMFS) was significantly higher in patients without retropharyngeal lymph node (RLN) metastasis than those with RLN metastasis (95.9% vs. 88.1% respectively, P = 0.04). For N0 disease, the 5-year overall survival (OS), local relapse-free survival (LRFS), nodal relapse-free survival (NRFS) and DMFS rates were 93.8%, 97.1%, 99.1% and 95.9%, respectively. For T1N0, T2N0, T3N0 and T4N0, OS was 97.8%, 100%, 93.8% and 76.9%, LRFS was 100%, 92.9%, 100% and 88.9% and DMFS was 96.6%, 90.9%, 100% and 93.3%, respectively. OS and LRFS were higher in T1-3 N0 patients than T4N0 patients (P < 0.01 and P = 0.01, respectively).
The seventh edition of the AJCC N-staging system improves prognostic accuracy by upgrading RLN metastasis to N1 disease. IMRT produces excellent survival rates in T1-3 N0 disease; however, T4N0 disease remains a challenge and additional improvements are required to achieve a favorable prognosis for these NPC patients.
调强适形放疗(IMRT)为鼻咽癌(NPC)提供了极好的局部区域控制,已逐渐取代二维常规放疗成为一线放疗技术。此外,在新的第七版美国癌症联合委员会(AJCC)分期系统中,由于咽后淋巴结(RLN)转移对 NPC 无远处转移生存(DMFS)率的负面影响,RLN 从 N0 期升级为 N1 期。本回顾性研究旨在探讨 IMRT 后 NPC 患者 N0 期的治疗结果和失败模式,以便为未来的治疗提供有效指导。
我们回顾性分析了 506 例经活检证实的非转移性 NPC 患者的数据。191 例患者无颈部淋巴结受累。根据第七版 AJCC 分期系统,110 例(21.7%)患者分期为 N0 期,81 例(16.0%)因 RLN 转移而重新分类为 N1 期。所有患者均接受 IMRT 作为主要治疗方法。
在无颈部淋巴结受累的患者中,无 RLN 转移患者的无远处转移生存(DMFS)明显高于 RLN 转移患者(分别为 95.9%和 88.1%,P=0.04)。对于 N0 期患者,5 年总生存率(OS)、局部无复发生存率(LRFS)、淋巴结无复发生存率(NRFS)和 DMFS 率分别为 93.8%、97.1%、99.1%和 95.9%。对于 T1N0、T2N0、T3N0 和 T4N0,OS 分别为 97.8%、100%、93.8%和 76.9%,LRFS 分别为 100%、92.9%、100%和 88.9%,DMFS 分别为 96.6%、90.9%、100%和 93.3%。T1-3 N0 患者的 OS 和 LRFS 均高于 T4N0 患者(P<0.01 和 P=0.01)。
第七版 AJCC N 分期系统通过将 RLN 转移升级为 N1 期,提高了预后准确性。IMRT 对 T1-3 N0 疾病产生了极好的生存率;然而,T4N0 疾病仍然是一个挑战,需要进一步改进以实现这些 NPC 患者的良好预后。