Department of Radiation Oncology, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou, 510060, Guangdong Province, People's Republic of China.
Department of Radiation Oncology, the Fifth Affiliated Hospital of Sun Yat-sen University, Zhuhai, 519001, Guangdong Province, China.
BMC Cancer. 2018 Jul 16;18(1):740. doi: 10.1186/s12885-018-4495-2.
Previous studies have reported radiotherapy interruption (RTI) is associated with poor local control in two-dimensional radiotherapy (2DRT) era. However, it remains unclear whether RTI still affects local control for advanced T stage (T3-4) in the intensity-modulated radiation therapy (IMRT) era. We aim to evaluate whether RTI affects local control for T3-4 NPC treated with definitive IMRT.
In this observational prospective study, 447 T3-4 NPC patients treated with IMRT plus concurrent chemotherapy were included. All patients completed the planned radiotherapy course, and RTI was defined as the actual time taken to finish the prescribed course of radiotherapy minus the planned radiotherapy time. Receiver operating characteristic (ROC) curve was used for determined the cutoff point of RTI. The effects of RTI on local control were analyzed in multivariate analysis.
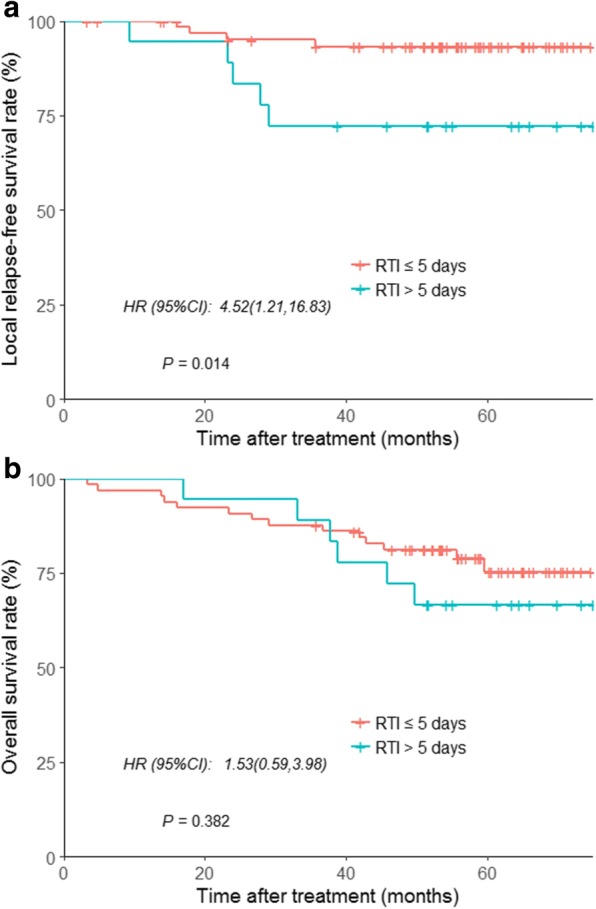
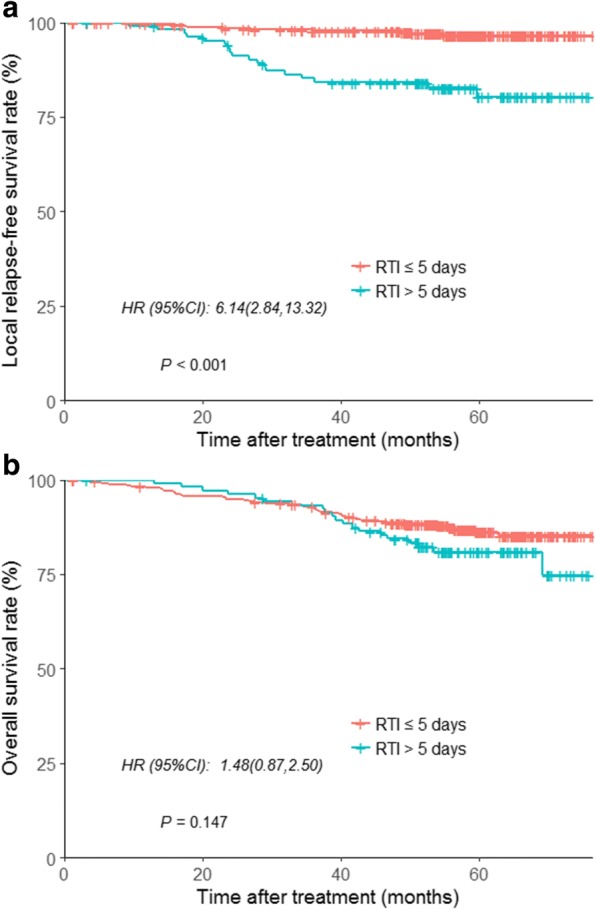
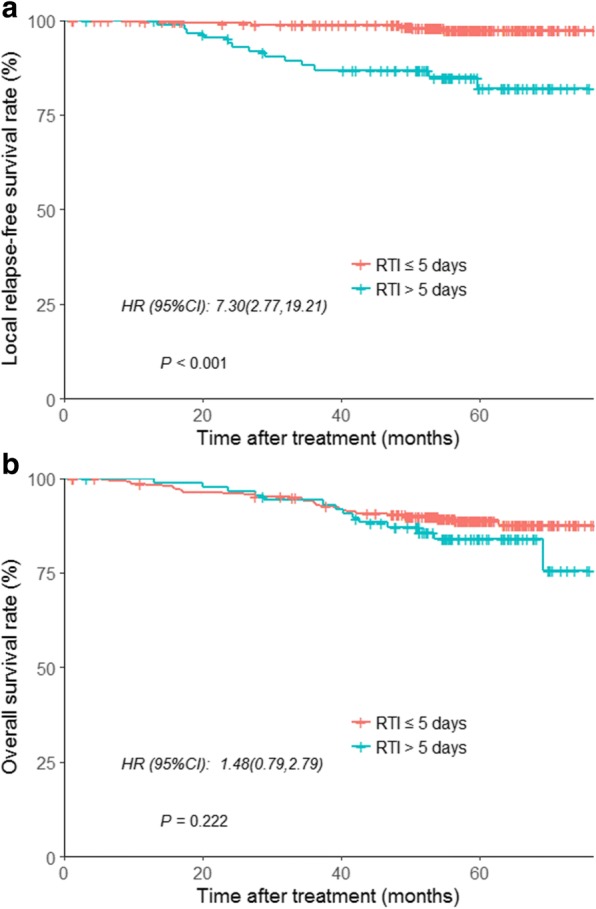
At 5 years, the local relapse-free survival (LRFS) and overall survival (OS) rates were 93.7 and 85.7%, respectively. The cutoff RTI for LRFS was 5.5 days by ROC curve. Compared to patients with RTI > 5 days, patients with RTI ≤ 5 days had a significantly lower rate of LRFS (97% vs. 83%; P < 0.001). In multivariate analysis, RTI was a risk factor independently associated with LRFS (HR = 9.64, 95% CI, 4.10-22.65), but not for OS (HR = 1.09, 95% CI, 0.84-1.64).
The current analysis demonstrates a significant correlation between prolonged RTI and local control in NPC, even when concurrent chemotherapy is used. We consider that attention to RTI seems to be warranted for patients with advanced T-stage NPC in the era of IMRT.
先前的研究报告称,在二维放射治疗(2DRT)时代,放疗中断(RTI)与局部控制不良有关。然而,在调强放射治疗(IMRT)时代,RTI 是否仍会影响 T3-4 期晚期鼻咽癌的局部控制尚不清楚。我们旨在评估在接受根治性 IMRT 治疗的 T3-4 期 NPC 患者中,RTI 是否会影响局部控制。
在这项观察性前瞻性研究中,纳入了 447 例接受 IMRT 加同期化疗的 T3-4 期 NPC 患者。所有患者均完成了计划的放疗疗程,RTI 定义为完成规定放疗疗程所需的实际时间减去计划放疗时间。受试者工作特征(ROC)曲线用于确定 RTI 的截断点。在多变量分析中分析了 RTI 对局部控制的影响。
在 5 年时,局部无复发生存率(LRFS)和总生存率(OS)分别为 93.7%和 85.7%。ROC 曲线确定的 LRFS 截断 RTI 为 5.5 天。与 RTI>5 天的患者相比,RTI≤5 天的患者 LRFS 率显著降低(97%比 83%;P<0.001)。在多变量分析中,RTI 是与 LRFS 独立相关的危险因素(HR=9.64,95%CI,4.10-22.65),但与 OS 无关(HR=1.09,95%CI,0.84-1.64)。
目前的分析表明,即使同时进行化疗,RTI 延长与 NPC 的局部控制之间存在显著相关性。我们认为,在 IMRT 时代,对于 T 期晚期 NPC 患者,关注 RTI 似乎是有必要的。