Department of General and Abdominal Surgery, Johannes Gutenberg University-Hospital of Mainz, Mainz, Germany.
BMC Cancer. 2012 Feb 15;12:70. doi: 10.1186/1471-2407-12-70.
Our aim was to compare survival of the various treatment modality groups of chemotherapy and/or radiotherapy in relation to SEMS (self-expanding metal stents) in a retrospective case-control study. We have made the hypothesis that the administration of combined chemoradiotherapy improves survival in inoperable esophageal cancer patients.
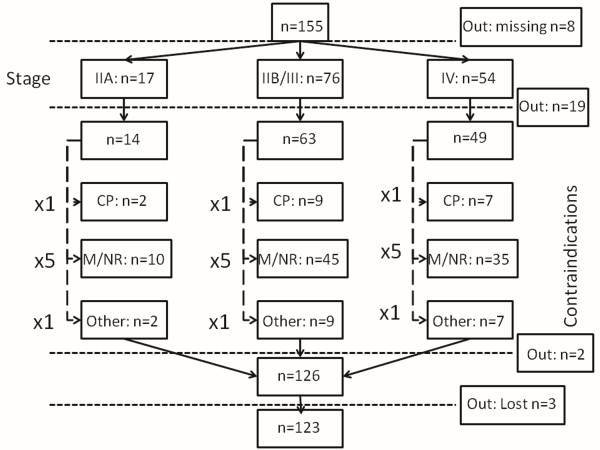
All patients were confirmed histologically as having surgically non- resectable esophageal carcinoma. Included were patients with squamous cell carcinoma, undifferentiated carcinoma as well as Siewert type I--but not type II - esophagogastric junctional adenocarcinoma. The decision to proceed with palliative treatments was taken within the context of a multidisciplinary team meeting and full expert review based on patient's wish, co-morbid disease, clinical metastases, distant metastases, M1 nodal metastases, T4-tumor airway, aorta, main stem bronchi, cardiac invasion, and peritoneal disease. Patients not fit enough to tolerate a radical course of definitive chemo- and/or radiation therapy were referred for self-expanding metal stent insertion. Our approach to deal with potential confounders was to match subjects according to their clinical characteristics (contraindications for surgery) and tumor stage according to diagnostic work-up in four groups: SEMS group (A), Chemotherapy group (B), Radiotherapy group (C), and Chemoradiotherapy group (D).
Esophagectomy was contraindicated in 155 (35.5%) out of 437 patients presenting with esophageal cancer to the Department of General and Abdominal Surgery of the University Hospital of Mainz, Germany, between November 1997 and November 2007. There were 133 males and 22 females with a median age of 64.3 (43-88) years. Out of 155 patients, 123 were assigned to four groups: SEMS group (A) n = 26, Chemotherapy group (B) n = 12, Radiotherapy group (C) n = 23 and Chemoradiotherapy group (D) n = 62. Mean patient survival for the 4 groups was as follows: Group A: 6.92 ± 8.4 months; Group B: 7.75 ± 6.6 months; Group C: 8.56 ± 9.5 months, and Group D: 13.53 ± 14.7 months. Significant differences in overall survival were associated with tumor histology (P = 0.027), tumor localization (P = 0.019), and type of therapy (P = 0.005), respectively, in univariate analysis. Treatment modality (P = 0.043) was the only independent predictor of survival in multivariate analysis. The difference in overall survival between Group A and Group D was highly significant (P < 0.01) and in favor of Group D. As concerns Group D versus Group B and Group D versus Group C there was a trend towards a difference in overall survival in favor of Group D (P = 0.069 and P = 0.059, respectively).
The prognosis of inoperable esophageal cancer seems to be highly dependent on the suitability of the induction of patient-specific therapeutic measures and is significantly better, when chemoradiotherapy is applied.
我们的目的是通过回顾性病例对照研究比较化疗和/或放疗的各种治疗方式组与支架(自膨式金属支架)的生存率。我们提出假设,联合放化疗可提高不可切除食管癌患者的生存率。
所有患者均经组织学证实为无法手术切除的食管癌。包括鳞状细胞癌、未分化癌以及 Siewert Ⅰ型-但不包括Ⅱ型-食管胃交界腺癌。姑息治疗的决策是在多学科团队会议和根据患者意愿、合并症、临床转移、远处转移、M1 淋巴结转移、T4 肿瘤气道、主动脉、主支气管、心脏侵犯和腹膜疾病进行的全面专家审查的背景下做出的。不适合接受根治性放化疗的患者被转介行自膨式金属支架置入术。我们处理潜在混杂因素的方法是根据他们的临床特征(手术禁忌)和根据诊断性检查确定的肿瘤分期将患者按以下四个组进行匹配:支架组(A)、化疗组(B)、放疗组(C)和放化疗组(D)。
1997 年 11 月至 2007 年 11 月,德国美因茨大学医院普外科共收治了 437 例食管癌患者,其中 155 例(35.5%)因手术禁忌而不能进行手术。其中男性 133 例,女性 22 例,中位年龄为 64.3(43-88)岁。在 155 例患者中,123 例被分配到四组:支架组(A)n=26 例,化疗组(B)n=12 例,放疗组(C)n=23 例,放化疗组(D)n=62 例。4 组患者的平均生存时间如下:A 组:6.92±8.4 个月;B 组:7.75±6.6 个月;C 组:8.56±9.5 个月;D 组:13.53±14.7 个月。单因素分析显示,肿瘤组织学(P=0.027)、肿瘤定位(P=0.019)和治疗类型(P=0.005)与总生存时间存在显著差异。多因素分析显示,治疗方式(P=0.043)是唯一的独立生存预测因素。A 组和 D 组之间的总生存差异具有统计学意义(P<0.01),且 D 组优于 A 组。至于 D 组与 B 组和 D 组与 C 组,D 组的总生存优势呈趋势(P=0.069 和 P=0.059)。
不可切除食管癌的预后似乎高度依赖于诱导患者特异性治疗措施的适宜性,当应用放化疗时,预后明显改善。
