Department of Neurology, Kantonsspital St. Gallen, St. Gallen, Switzerland.
PLoS One. 2012;7(2):e31275. doi: 10.1371/journal.pone.0031275. Epub 2012 Feb 20.
Neuroanatomical determinants of motor skill recovery after stroke are still poorly understood. Although lesion load onto the corticospinal tract is known to affect recovery, less is known about the effect of lesions to cortical sensorimotor areas. Here, we test the hypothesis that lesions of somatosensory cortices interfere with the capacity to recover motor skills after stroke.
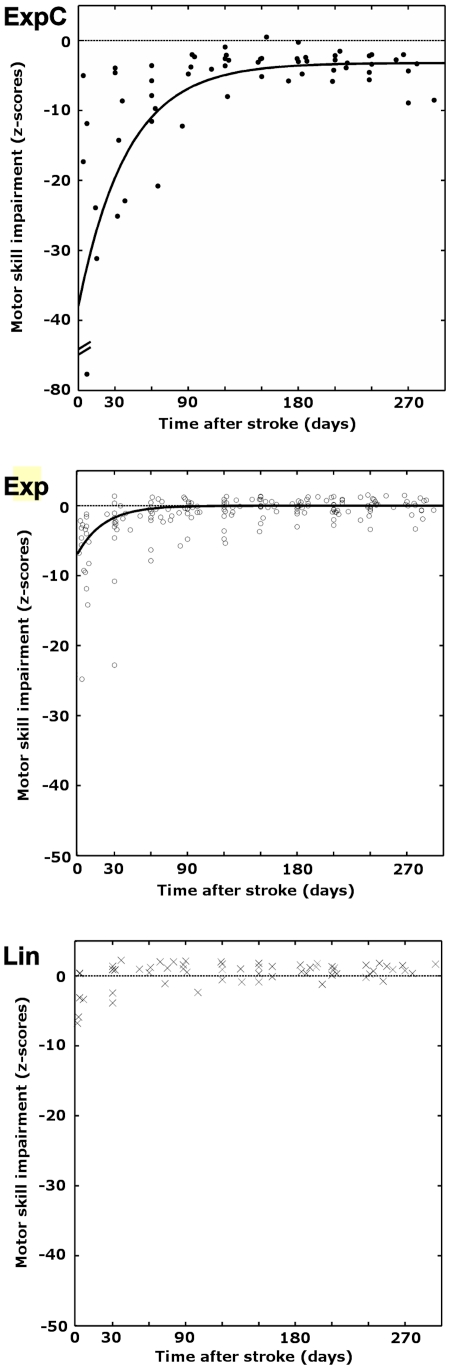
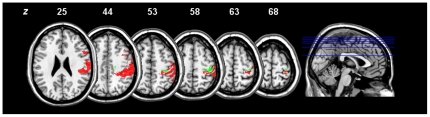
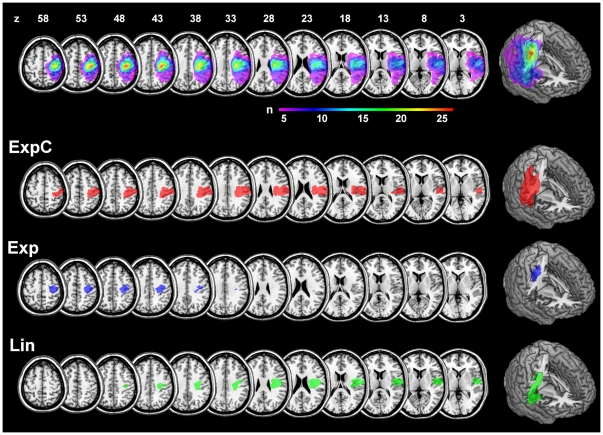
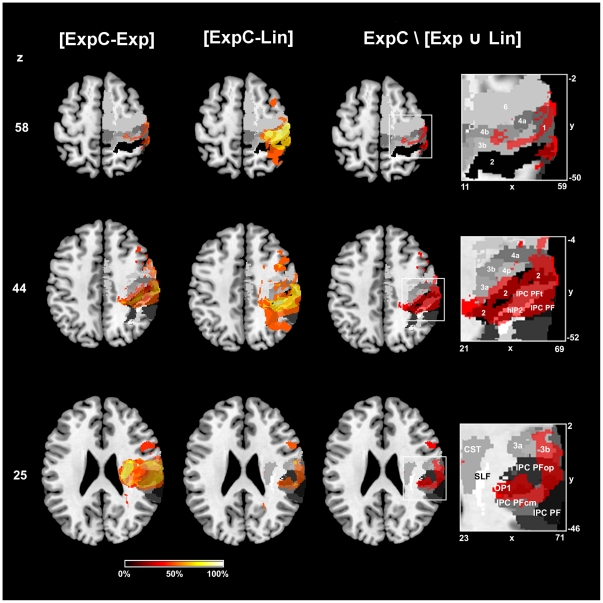
Standardized tests of motor skill and somatosensory functions were acquired longitudinally over nine months in 29 patients with stroke to the pre- and postcentral gyrus, including adjacent areas of the frontal, parietal and insular cortices. We derived the recovery trajectories of each patient for five motor subtest using least-squares curve fitting and objective model selection procedures for linear and exponential models. Patients were classified into subgroups based on their motor recovery models. Lesions were mapped onto diffusion weighted imaging scans and normalized into stereotaxic space using cost-function masking. To identify critical neuranatomical regions, voxel-wise subtractions were calculated between subgroup lesion maps. A probabilistic cytoarchitectonic atlas was used to quantify of lesion extent and location.
Twenty-three patients with moderate to severe initial deficits showed exponential recovery trajectories for motor subtests that relied on precise distal movements. Those that retained a chronic motor deficit had lesions that extended to the center of the somatosensory cortex (area 2) and the intraparietal sulcus (areas hIP1, hIP2). Impaired recovery outcome correlated with lesion extent on this areas and somatosensory performance. The rate of recovery, however, depended on the lesion load onto the primary motor cortex (areas 4a, 4p).
Our findings support a critical role of uni-and multimodal somatosensory cortices in motor skill recovery. Whereas lesions to these areas influence recovery outcome, lesions to the primary motor cortex affect recovery dynamics. This points to a possible dissociation of neural substrates for different aspects of post-stroke recovery.
中风后运动技能恢复的神经解剖学决定因素仍知之甚少。虽然皮质脊髓束的病变负荷已知会影响恢复,但皮质感觉运动区病变的影响知之甚少。在这里,我们测试了这样一个假设,即感觉皮质的病变会干扰中风后运动技能的恢复能力。
对 29 名中风患者的感觉运动皮质进行了为期 9 个月的标准化运动技能和感觉功能的纵向测试,包括额、顶和岛叶皮质的前中央回和相邻区域。我们使用最小二乘法曲线拟合和线性和指数模型的客观模型选择程序,为五个运动子测试推导出每个患者的恢复轨迹。根据运动恢复模型将患者分为亚组。将病变映射到弥散加权成像扫描中,并使用成本函数掩模将其归一化为立体定向空间。为了识别关键的神经解剖区域,在亚组病变图之间进行了体素减法计算。使用概率细胞构筑学图谱来量化病变的范围和位置。
23 名初始缺陷程度为中度至重度的患者表现出依赖于精确的远端运动的运动子测试的指数恢复轨迹。那些保留慢性运动缺陷的患者的病变延伸到感觉皮质的中心(区域 2)和顶内沟(区域 hIP1、hIP2)。受损的恢复结果与这些区域和感觉性能的病变程度相关。然而,恢复速度取决于初级运动皮质(区域 4a、4p)的病变负荷。
我们的研究结果支持单一和多模态感觉皮质在运动技能恢复中的关键作用。虽然这些区域的病变会影响恢复结果,但初级运动皮质的病变会影响恢复动态。这表明中风后恢复的不同方面的神经基础可能存在分离。