Atkinson Elizabeth J, Therneau Terry M, Melton L Joseph, Camp Jon J, Achenbach Sara J, Amin Shreyasee, Khosta Sundeep
Divisions of Biomedical Statistics and Informatics, College of Medicine, Mayo Clinic, Rochester, MN, USA.
J Bone Miner Res. 2012 Jun;27(6):1397-404. doi: 10.1002/jbmr.1577.
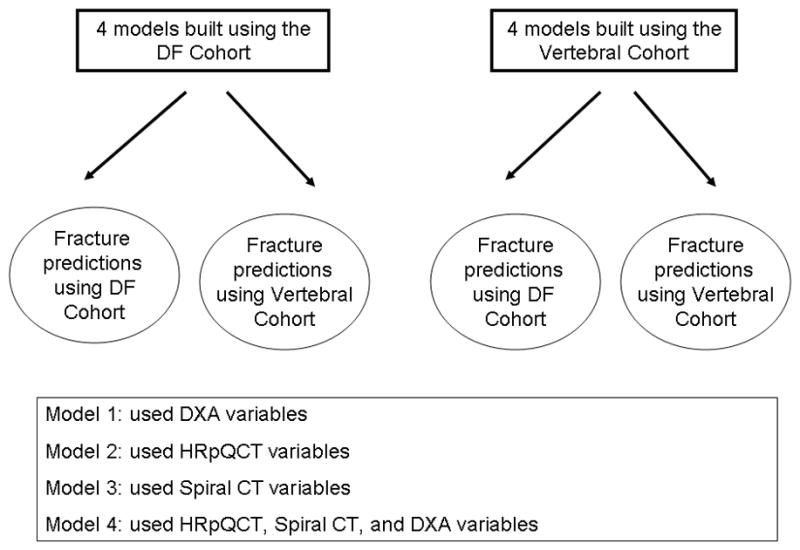
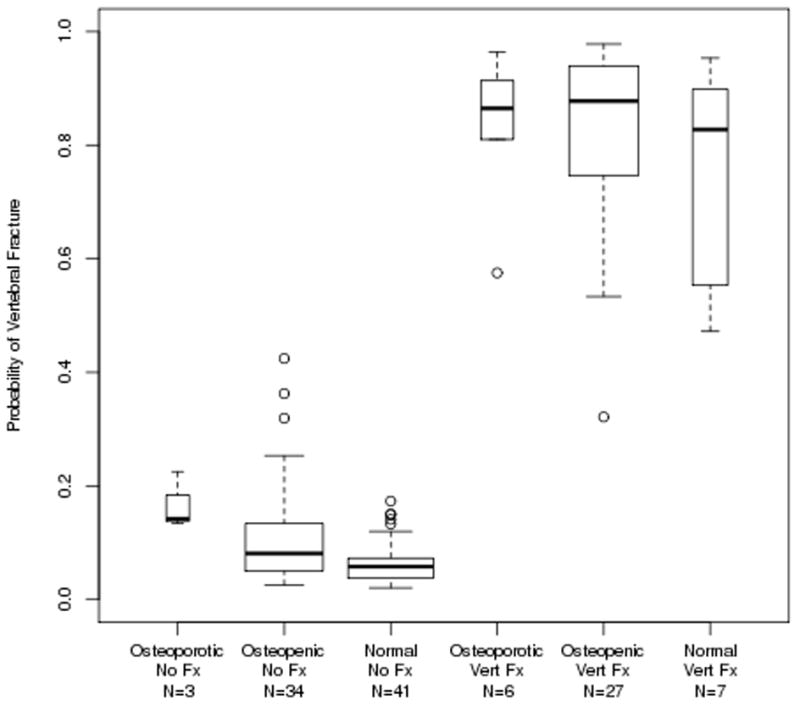
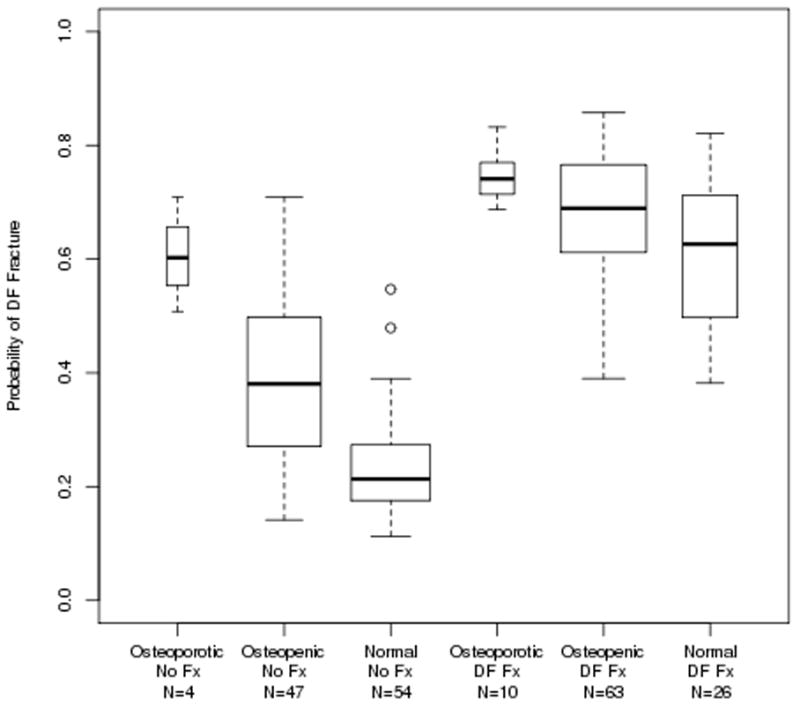
Advanced bone imaging with quantitative computed tomography (QCT) has had limited success in significantly improving fracture prediction beyond standard areal bone mineral density (aBMD) measurements. Thus, we examined whether a machine learning paradigm, gradient boosting machine (GBM) modeling, which can incorporate diverse measurements of bone density and geometry from central QCT imaging and of bone microstructure from high-resolution peripheral QCT imaging, can improve fracture prediction. We studied two cohorts of postmenopausal women: 105 with and 99 without distal forearm fractures (Distal Forearm Cohort) and 40 with at least one grade 2 or 3 vertebral deformity and 78 with no vertebral fracture (Vertebral Cohort). Within each cohort, individual bone density, structure, or strength variables had areas under receiver operating characteristic curves (AUCs) ranging from 0.50 to 0.84 (median 0.61) for discriminating women with and without fracture. Using all possible variables in the GBM model, the AUCs were close to 1.0. Fracture predictions in the Vertebral Cohort using the GBM models built with the Distal Forearm Cohort had AUCs of 0.82-0.95, while predictions in the Distal Forearm Cohort using models built with the Vertebral Cohort had AUCs of 0.80-0.83. Attempts at capturing a comparable parametric model using the top variables from the Distal Forearm Cohort resulted in resulted in an AUC of 0.81. Relatively high AUCs for differing fracture types suggest that an underlying fracture propensity is being captured by this modeling approach. More complex modeling, such as with GBM, creates stronger fracture predictions and may allow deeper insights into information provided by advanced bone imaging techniques.
与标准的面积骨密度(aBMD)测量相比,采用定量计算机断层扫描(QCT)的先进骨成像技术在显著改善骨折预测方面成效有限。因此,我们研究了一种机器学习范式——梯度提升机(GBM)建模,它可以整合来自中央QCT成像的骨密度和几何结构的各种测量数据以及来自高分辨率外周QCT成像的骨微结构测量数据,是否能够改善骨折预测。我们研究了两组绝经后女性:105名有和99名无桡骨远端骨折的女性(桡骨远端骨折队列),以及40名至少有一处2级或3级椎体畸形和78名无椎体骨折的女性(椎体队列)。在每个队列中,用于区分有骨折和无骨折女性的个体骨密度、结构或强度变量的受试者操作特征曲线(AUC)范围为0.50至0.84(中位数为0.61)。在GBM模型中使用所有可能的变量时,AUC接近1.0。使用基于桡骨远端骨折队列构建的GBM模型对椎体队列进行骨折预测时,AUC为0.82 - 0.95,而使用基于椎体队列构建的模型对桡骨远端骨折队列进行预测时,AUC为0.80 - 0.83。尝试使用桡骨远端骨折队列中的顶级变量来构建一个可比的参数模型,得到的AUC为0.81。不同骨折类型的相对较高AUC表明这种建模方法捕捉到了潜在的骨折倾向。更复杂的建模,如GBM,能产生更强的骨折预测,并可能使我们对先进骨成像技术提供的信息有更深入的了解。