Kristiansen Hm, Hovstad T, Vollan G, Faerestrand S
Department of Heart Disease, Haukeland University Hospital, Bergen, Norway.
Indian Pacing Electrophysiol J. 2012 Jan;12(1):4-14. doi: 10.1016/s0972-6292(16)30458-2. Epub 2012 Jan 31.
The conventional right ventricular (RV) lead position in cardiac resynchronization therapy pacemakers (CRT-P) is the RV apex (RV-A). Little is known about electrophysiological stability and associated complications of pacing leads in RV high posterior septal (RV-HS) position in CRT-P.
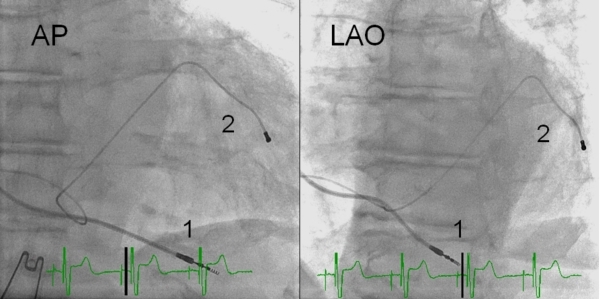
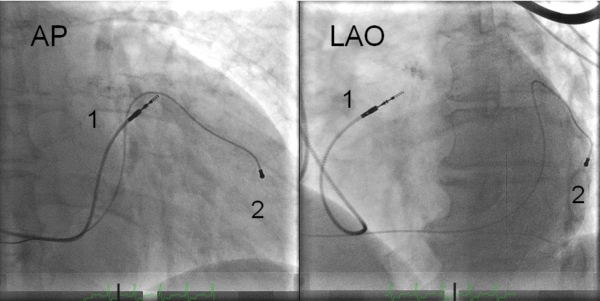
Two hundred and thirty-five consecutive CRT-P patients were included from 1999-2010. Pacing thresholds at 0.5ms and 2.5V, sensing electrograms and lead impedances were measured at implant and repeated 1,3,6,12,18 and 24 months after CRT-P. Electrophysiological measurements of leads located in RV-A and RV-HS were analyzed retrospectively. Bipolar RV leads were used, including high impedance leads, passive fixation and active fixation.
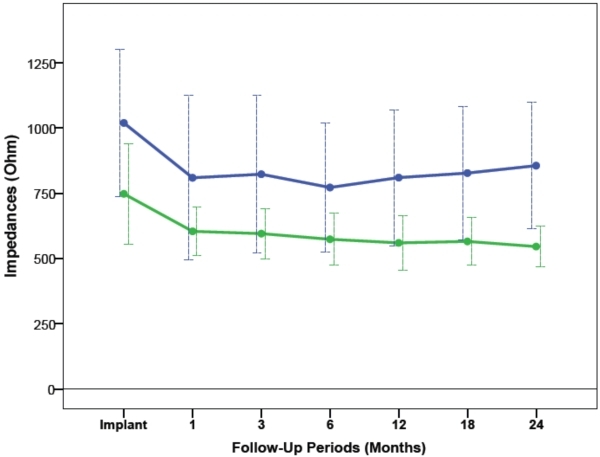
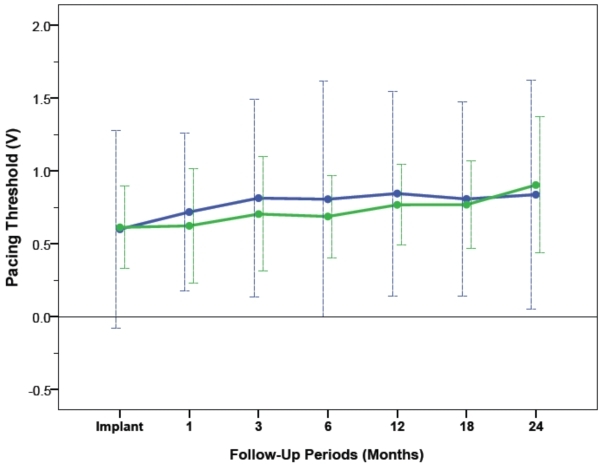
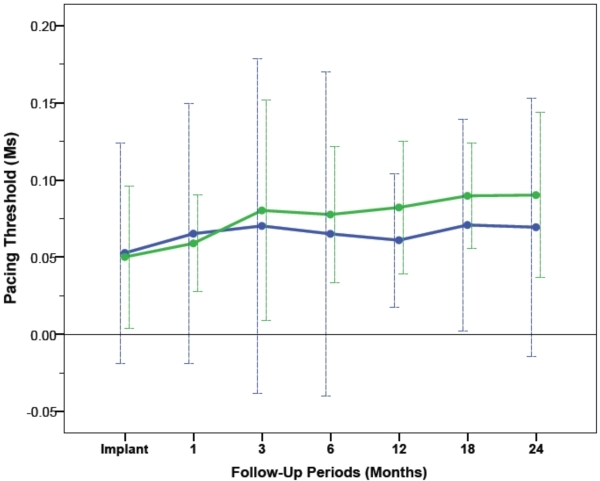
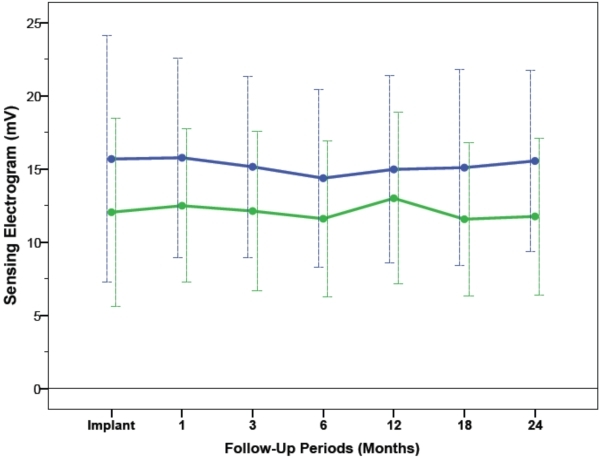
RV pacing leads were implanted in RV-A (n=79) and RV-HS (n=156). Average RV pacing thresholds from CRT implant procedure to 24-month follow-up at 0.5ms were 0.77±0.69V in RV-A and 0.71±0.35V in RV-HS (P=0.31), and at 2.5V were 0.06±0.08ms in RV-A and 0.07±0.05ms in RV-HS (P=0.12). Average RV electrogram amplitudes from baseline to 24 months after CRT were 15.3±6.9mV in RV-A and 12.1±6.0mV in RV-HS (P=0.55). Average RV impedances during follow-up were 850±286Ω in RV-A and 618±147Ω in RV-HS (P=0.57). Similar RV lead revisions between RV-A and RV-HS were observed after 2-year follow-up (P=0.55).
The RV-HS lead position demonstrated stable and acceptable long-term pacing and sensing function, with rates of complications comparable to conventional RV-A lead position in CRT. The RV-HS lead position is feasible in CRT-P.
心脏再同步治疗起搏器(CRT-P)中传统的右心室(RV)导联位置是右心室心尖部(RV-A)。关于CRT-P中右心室高后间隔(RV-HS)位置起搏导线的电生理稳定性及相关并发症,人们了解甚少。
纳入1999年至2010年连续的235例CRT-P患者。在植入时及CRT-P植入后1、3、6、12、18和24个月测量0.5ms和2.5V时的起搏阈值、感知电图和导线阻抗。对位于RV-A和RV-HS的导线的电生理测量进行回顾性分析。使用双极RV导线,包括高阻抗导线、被动固定和主动固定导线。
RV起搏导线分别植入RV-A(n = 79)和RV-HS(n = 156)。从CRT植入手术到24个月随访,0.5ms时RV-A的平均RV起搏阈值为0.77±0.69V,RV-HS为0.71±0.35V(P = 0.31);2.5V时,RV-A为0.06±0.08ms,RV-HS为0.07±0.05ms(P = 0.12)。从基线到CRT后24个月,RV-A的平均RV电图振幅为15.3±6.9mV,RV-HS为12.1±6.0mV(P = 0.55)。随访期间,RV-A的平均RV阻抗为850±286Ω,RV-HS为618±147Ω(P = 0.57)。两年随访后,RV-A和RV-HS之间观察到相似的RV导线修订率(P = 0.55)。
RV-HS导线位置显示出稳定且可接受的长期起搏和感知功能,并发症发生率与CRT中传统的RV-A导线位置相当。RV-HS导线位置在CRT-P中是可行的。